Thoracic Endovascular Repair of Spinal Cord Infarction Resulting from Impending Rupture of the Thoracic Aortic Aneurysm
- Affiliations
-
- 1Department of Thoracic and Cardiovascular Surgery, Jeju National University School of Medicine, Jeju, Korea.
- 2Department of Radiology, Jeju National University School of Medicine, Jeju, Korea.
- 3Department of Neurology, Jeju National University School of Medicine, Jeju, Korea. oh.junghwan77@gmail.com
- KMID: 2434844
- DOI: http://doi.org/10.18700/jnc.180071
Abstract
- No abstract available.
Figure
-
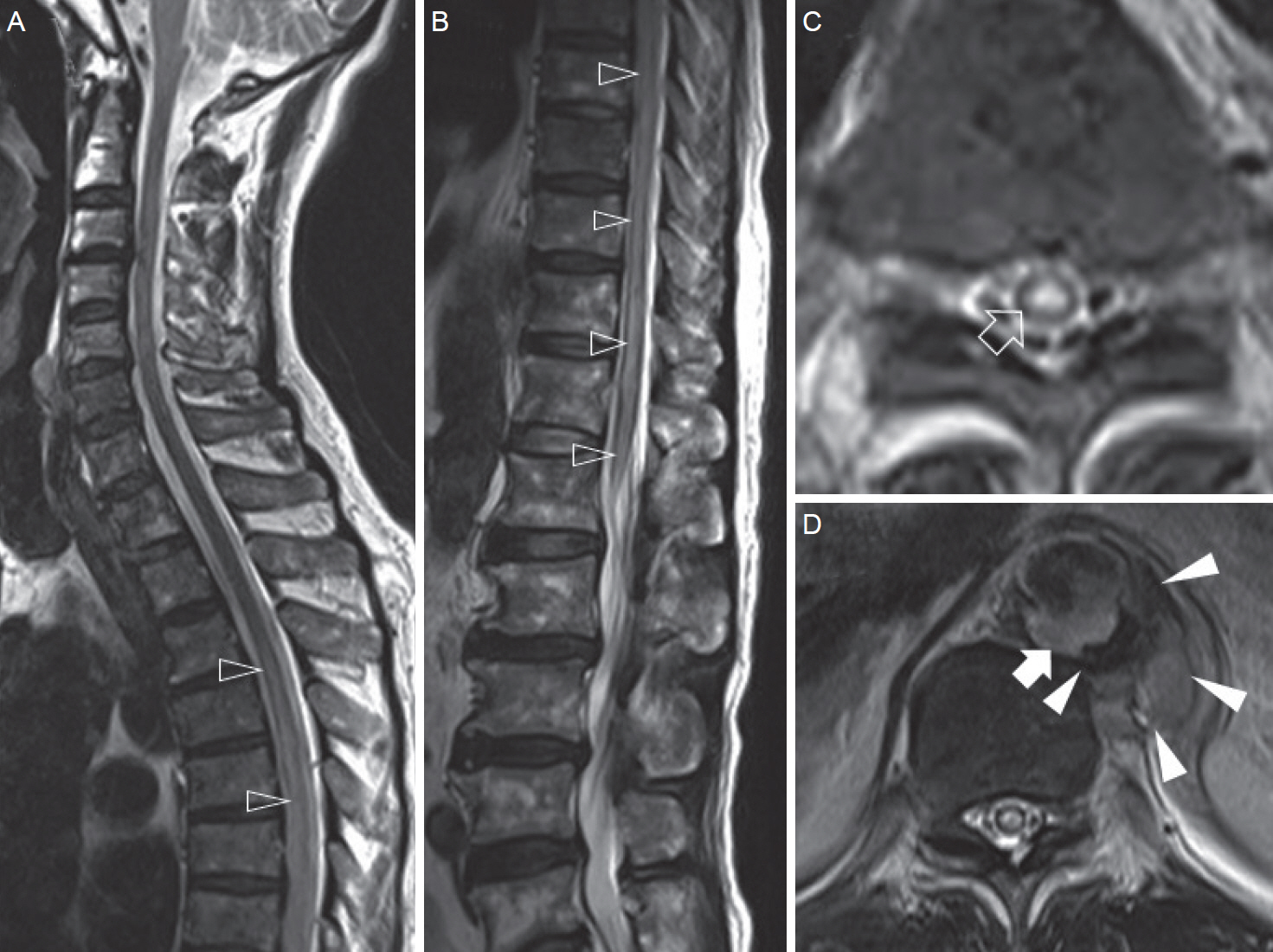
Figure 1. Initial findings of magnetic resolution imaging. T2-weighted sagittal views of the spinal cords showing diffuse high signal intensity with swelling (open arrowheads) from the T3 spinal cord to the conus medullaris (A, B). T2-weighted axial view at the T11 spinal cord (C), showing diffuse high signal intensity, involving the entire cross-section of the spinal cord (open arrow). Increased signal intensity in the mass-like lesion (closed arrow) in posterior wall of the distal thoracic aorta, revealing a penetrating aortic ulcer with heterogeneous signal intensity lesion, suggestive of surrounding hematoma (closed arrowheads) at the T10 level (D).

Figure 2. Findings of CTA. Initial CTA demonstrating a penetrating aortic ulcer (black arrow) with hematoma (white arrow), revealing impending rupture of the aorta (A) which is shown as an aneurysm (open arrow) on the 3D-image (B) at the of T10-11 spinal cord levels. Disappearance of penetrating aortic ulcer, and decreased size of aneurysm (open arrowhead) and hematoma (white arrowhead) on follow-up CTA one month after thoracic endovascular aortic repair (C, D). CTA, computed tomography angiography.
Reference
-
1. Romi F, Naess H. Spinal cord infarction in clinical neurology: a review of characteristics and long-term prognosis in comparison to cerebral infarction. Eur Neurol. 2016; 76:95–8.
Article2. Salvador de la Barrera S, Barca-Buyo A, Montoto-Marqués A, Ferreiro-Velasco ME, Cidoncha-Dans M, Rodriguez-Sotillo A. Spinal cord infarction: prognosis and recovery in a series of 36 patients. Spinal Cord. 2001; 39:520–5.
Article3. Hayashi H, Matsuoka Y, Sakamoto I, Sueyoshi E, Okimoto T, Hayashi K, et al. Penetrating atherosclerotic ulcer of the aorta: imaging features and disease concept. Radiographics. 2000; 20:995–1005.
Article4. Prince EA, Ahn SH. Basic vascular neuroanatomy of the brain and spine: what the general interventional radiologist needs to know. Semin Intervent Radiol. 2013; 30:234–9.
Article5. Mawad ME, Rivera V, Crawford S, Ramirez A, Breitbach W. Spinal cord ischemia after resection of thoracoabdominal aortic aneurysms: MR findings in 24 patients. AJR Am J Roentgenol. 1990; 155:1303–7.
Article6. Dake MD, Miller DC, Semba CP, Mitchell RS, Walker PJ, Liddell RP. Transluminal placement of endovascular stent-grafts for the treatment of descending thoracic aortic aneurysms. N Engl J Med. 1994; 331:1729–34.
Article7. Kim JT, Baek WK, Yoon YH, Kim YS, Shinn HK, Jeon YS, et al. Endovascular stent graft treatment in thoracic aortic aneurysmal disease. Korean J Vasc Endovasc Surg. 2013; 29:1–5.
Article8. Svensson LG, Kouchoukos NT, Miller DC, Bavaria JE, Coselli JS, Curi MA, et al. Expert consensus document on the treatment of descending thoracic aortic disease using endovascular stent-grafts. Ann Thorac Surg. 2008; 85(1 Suppl):S1–41.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Simultaneous Endovascular Aneurysm Repair for Abdominal Aortic Aneurysm Combined with Saccular Thoracic Aortic Aneurysm
- Endovascular Repair of Thoracic Aortic Aneurysm Using a Custom-made Fenestrated Stent Graft to Preserve the Left Subclavian Artery
- A Case of Paraplegia Following Endovascular Stent Repair of Descending Thoracic Aortic Aneurysm
- Long Segment Spinal Cord Infarction after Thoracic Endovascular Aortic Repair Implementation
- Retrograde Aortic Dissection after Thoracic Endovascular Aortic Repair for Descending Aorta: 2 case reports
