Analysis of Congenital Postaxial Polydactyly of the Foot Using Magnetic Resonance Imagings
- Affiliations
-
- 1W Institute for Congenital Limb Deformity, W Hospital, Daegu, Korea.
- 2Department of Orthopedic Surgery, Inje University Ilsan Paik Hospital, Goyang, Korea. osddr8151@paik.ac.kr
- KMID: 2430060
- DOI: http://doi.org/10.4055/jkoa.2018.53.6.530
Abstract
- PURPOSE
We aimed to evaluate the magnetic resonance imaging (MRI) findings of congenital postaxial polydactyly of the foot.
MATERIALS AND METHODS
Three-hundred and forty-seven feet of 288 patients who underwent congenital postaxial polydactyly or polysyndactyly correction were divided into five subtypes according to the radiographic shapes of deformity origins (widened metatarsal head, bifid, fused duplicated, incompletely duplicated, or completely duplicated). MRIs were assessed to determine whether they unrevealed areas were fused or separated. MRI was also used to assess cases with radiographic phalangeal aplasia.
RESULTS
Huge variations were noted in MRIs. Fusion or separation at the base or head between original and extra digits were observed, and MRI effectively depicted phalangeal aplastic areas.
CONCLUSION
MRI evaluations of congenital postaxial polydactyly of the foot are useful for determining the anatomical statuses which were not visualized by plain radiography (level of evidence: 3).
MeSH Terms
Figure
-

Figure 1 Four zones of radiographic deformity from proximal to distal.
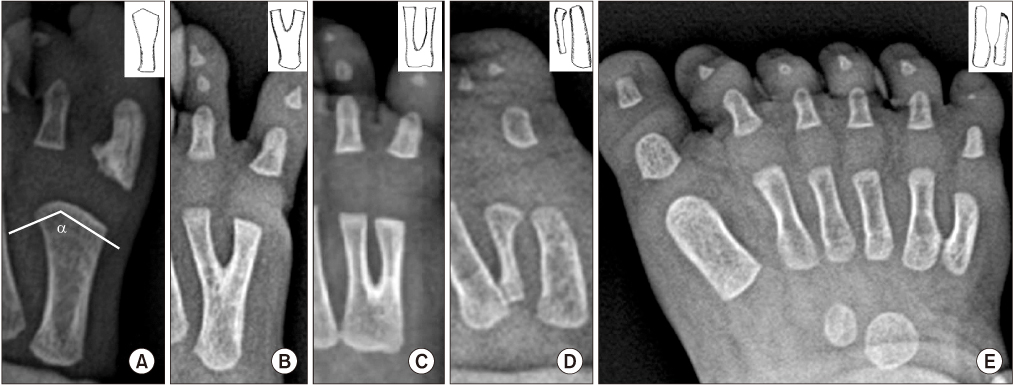
Figure 2 Five different deformity types. (A) The angle between two separate articular surfaces (a angle) was measured for the widened metatarsal head type. Bifid type was defined as sharing area of more than 50% of entire metatarsal length (B), and the fused duplicated type was defined as sharing less than 50% (C). Hypoplasia was used to differentiate the incompletely (D) and completely (E) duplicated types.
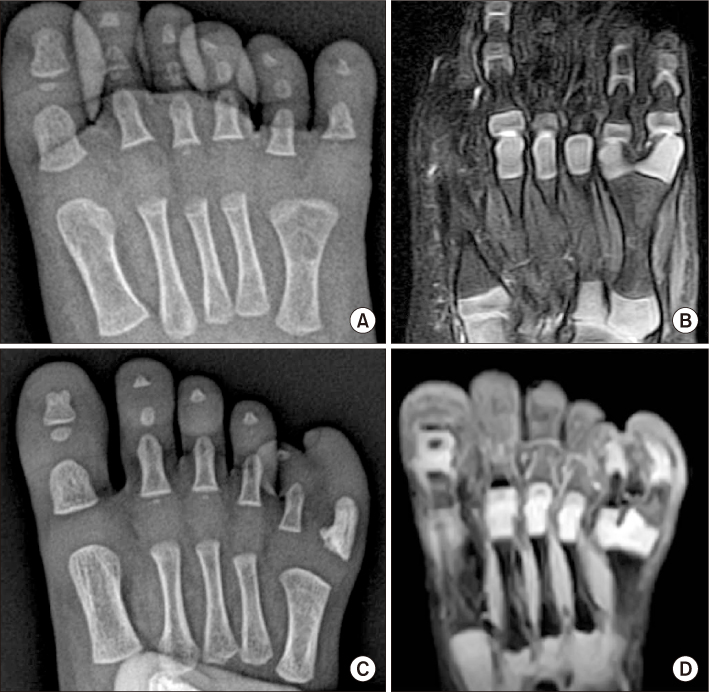
Figure 3 Two different patients showed similar radiographic findings of widened metatarsal head type polydactyly (A, C). However, magnetic resonance imagings revealed separation of the metatarsal head in one (B) and fusion in the other (D).

Figure 4 Radiograph of an 18-month-old male patient showing non-visualization of the middle phalanx (A), whereas magnetic resonance imagings (MRIs) showed two distinctly separate middle phalanges (B). Radiograph of an 11-month-old female patient showing one middle phalanx (C), whereas MRIs showed two with proximal fusion (D).
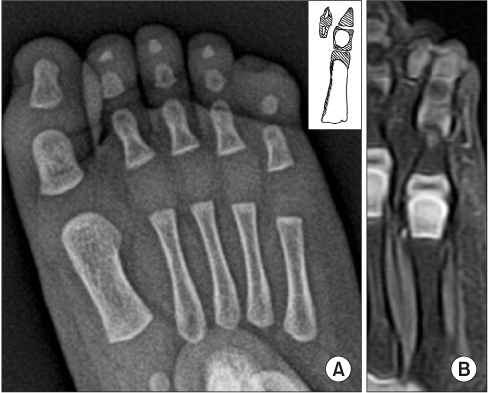
Figure 5 Aplasia of the distal phalanx was suspected based on radiographic findings (A), whereas magnetic resonance imaging showed incompletely duplicated type polydactyly of the distal phalanx (B).
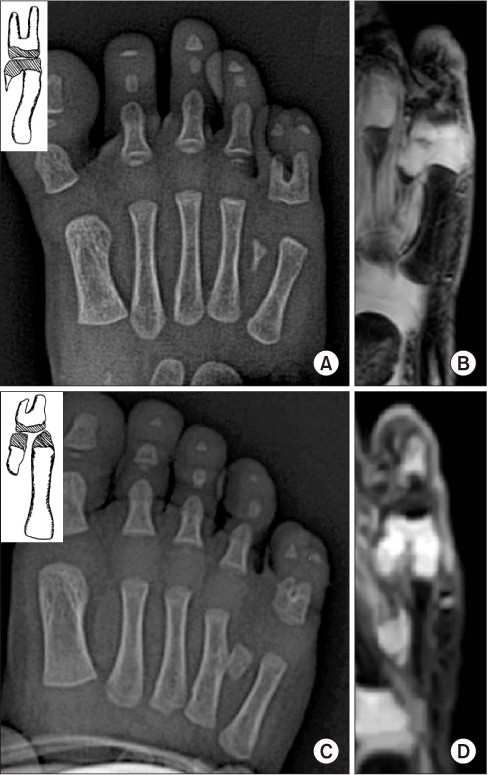
Figure 6 Radiographs of two patients (A, C) showed similar complex type polydactylies (incomplete duplication at the metatarsal level and fused duplication at the proximal phalanx). However, magnetic resonance imaging revealed different findings at metatarsal heads (B: fusion, D: separation), while bases of proximal phalanges were fused in both patients.
Reference
-
1. Miura T, Nakamura R, Imamura T. Polydactyly of the hands and feet. J Hand Surg Am. 1987; 12:474–476.
Article2. Son WG, Kwon ST, Lee SW. Simple classification of foot polydactyly based on the status of metatarsal bone and varus deformity. J Korean Soc Plast Reconstr Surg. 2004; 31:501–505.3. Nogami H. Polydactyly and polysyndactyly of the fifth toe. Clin Orthop Relat Res. 1986; 204:261–265.
Article4. Venn-Watson EA. Problems in polydactyly of the foot. Orthop Clin North Am. 1976; 7:909–927.
Article5. Wassel HD. The results of surgery for polydactyly of the thumb. a review. Clin Orthop Relat Res. 1969; 64:175–193.6. Lee HS, Park SS, Yoon JO, Kim JS, Youm YS. Classification of postaxial polydactyly of the foot. Foot Ankle Int. 2006; 27:356–362.
Article7. Seok HH, Park JU, Kwon ST. New classification of polydactyly of the foot on the basis of syndactylism, axis deviation, and metatarsal extent of extra digit. Arch Plast Surg. 2013; 40:232–237.
Article8. Konno M, Hirase Y. A clinical review of polydactyly in the foot and postoperative results of lateral ray polydactyly. J Jpn Soc Plast Reconstr Surg. 1997; 17:211–225.9. Watanabe H, Fujita S, Oka I. Polydactyly of the foot: an analysis of 265 cases and a morphological classification. Plast Reconstr Surg. 1992; 89:856–877.10. Hefti F, Brunner R, Hasler CC, Jundt G. Pediatric orthopedics in practice. Heidelberg: Springer Medizin;2007.11. Patel P. Pediatric foot and ankle. In : Parekh SG, editor. Foot and ankle surgery. New Delhi: Jaypee Brothers Medical Publishers;2012. p. 468–469.12. Kawabata H, Tada K, Masada K, Kawai H, Ono K. Revision of residual deformities after operations for duplication of the thumb. J Bone Joint Surg Am. 1990; 72:988–998.
Article13. Phelps DA, Grogan DP. Polydactyly of the foot. J Pediatr Orthop. 1985; 5:446–451.
Article14. Uda H, Sugawara Y, Niu A, Sarukawa S. Treatment of lateralray polydactyly of the foot: focusing on the selection of the toe to be excised. Plast Reconstr Surg. 2002; 109:1581–1591.15. Filges I, Kang A, Hench J, et al. Fetal polydactyly: a study of 24 cases ascertained by prenatal sonography. J Ultrasound Med. 2011; 30:1021–1029.16. Ermito S, Dinatale A, Carrara S, Cavaliere A, Imbruglia L, Recupero S. Prenatal diagnosis of limb abnormalities: role of fetal ultrasonography. J Prenat Med. 2009; 3:18–22.
