Case of Renal Microaneurysms and Multiple Renal Infarctions in a Patient with Systemic Lupus Erythematosus
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Kyungpook National University, Daegu, Korea. ejnam@knu.ac.kr
- 2Department of Pathology, School of Medicine, Kyungpook National University, Daegu, Korea.
- KMID: 2429714
- DOI: http://doi.org/10.4078/jrd.2018.25.4.296
Abstract
- Systemic lupus erythematosus (SLE) is a chronic inflammatory, heterogeneous autoimmune disease characterized by autoantibody production and the potential involvement of almost every organ system. Although vasculitis usually confined to small vessels is a fairly common feature of SLE, ischemic vasculitis with an aneurysm is an uncommon feature. In particular, renal arterial microaneurysms and multiple renal infarctions are very rarely reported in patients with SLE. Furthermore, to the best of the authors' knowledge, there is no report on renal arterial microaneurysms associated with SLE in Korea. Here, this paper presents a case of renal microaneurysms and multiple renal infarctions in a 41-year-old woman with SLE.
MeSH Terms
Figure
-

Figure 1 (A) Any abnormal lesions, such as lung nodule, parenchymal infiltration or cavities were not found on chest X-ray. (B) Water's view showed no abnormal haziness or opacification of the maxillary sinus. (C) Bone scan demonstrated an increase in uptake of the first to fifth metatarsophalangeal joints on left foot (arrows). (D) Foot X-ray did not reveal any erosions on metatarsophalangeal joints of both feet.
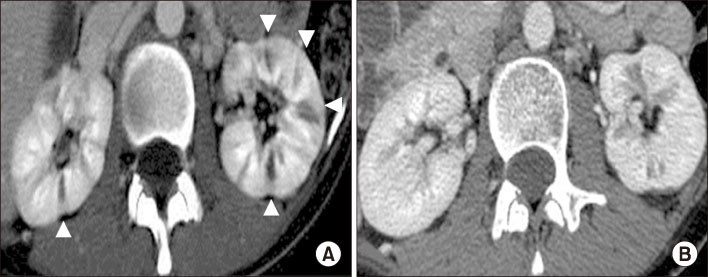
Figure 2 (A) Abdominal computed tomography (CT) revealed multiple wedge-shaped, sharply marginated, low-density lesions (arrowheads) in the both kidney parenchyma, which are consisted with the findings of renal infarctions. (B) After ten months of therapy, follow-up abdominal CT showed improved lesions in the both renal parenchyma.
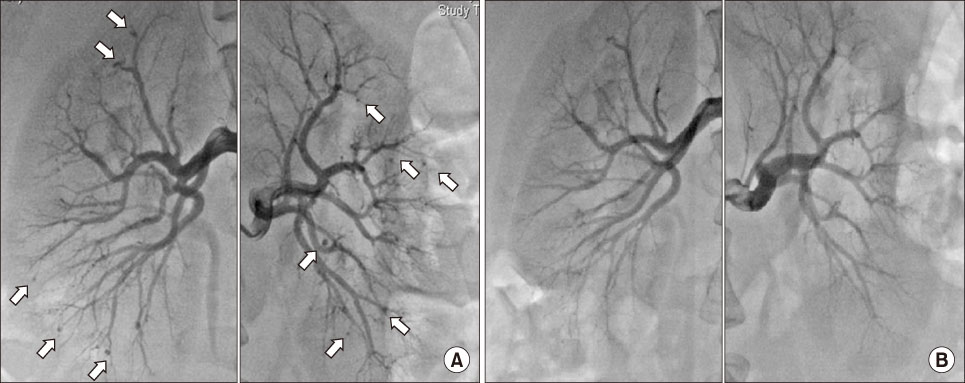
Figure 3 (A) Renal angiograpy showed multiple saccular microaneurysms in the peripheral segments of the right and left renal arteries. (B) After ten months of therapy, follow-up renal angiography showed a significantly reduced number of microaneurysms.
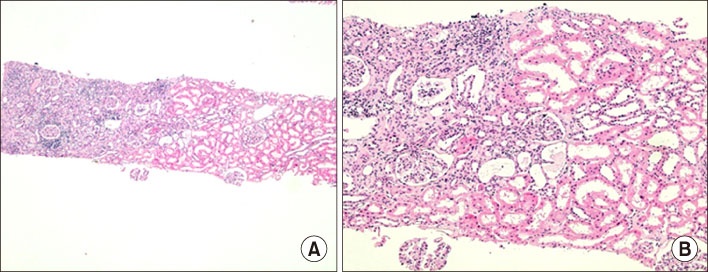
Figure 4 Histopathologic analysis of kidney demonstrated well-demarcated atrophic change and scar formation with prominent peritubular inflammatory cell infiltrations. However, there were no evidences of a fibrinoid necrosis of vascular beds or active glomerular lesions (H&E, A: ×40, B: ×100).
Reference
-
1. Ramos-Casals M, Nardi N, Lagrutta M, Brito-Zeron P, Bove A, Delgado G, et al. Vasculitis in systemic lupus erythematosus: prevalence and clinical characteristics in 670 patients. Medicine (Baltimore). 2006; 85:95–104.2. Pyrpasopoulou A, Chatzimichailidou S, Aslanidis S. Vascular disease in systemic lupus erythematosus. Autoimmune Dis. 2012; 2012:876456.
Article3. Radic M, Martinovic Kaliterna D, Radic J. Vascular manifestations of systemic lupus erythematosis. Neth J Med. 2013; 71:10–16.4. Vitali C, Bencivelli W, Isenberg DA, Smolen JS, Snaith ML, Sciuto M, et al. Disease activity in systemic lupus erythematosus: report of the Consensus Study Group of the European Workshop for Rheumatology Research. I. A descriptive analysis of 704 european lupus patients. European Consensus Study Group for disease activity in SLE. Clin Exp Rheumatol. 1992; 10:527–539.5. Drekard C, Villa AR, Reyes E, Abello M, Alarcon-Segovia D. Vasculitis in systemic lupus erythematosus. Lupus. 1997; 6:235–242.
Article6. Sánchez-Ojanguren J, Matias J, Misis M, Olivé A. Systemic lupus erythematosus, berry aneurysm and subarachnoid haemorrhage. Clin Rheumatol. 1999; 18:165–166.
Article7. Yamazaki K. Systemic lupus erythematosus with hepatic aneurysm, valsalva sinus aneurysm and associated polyangiitis: aneurysmal wall remodeling with dense fibrosis and calcification mediated by residual smooth muscle cells. Lupus. 2004; 13:54–59.8. Tsai YG, Lai JH, Kuo SY, Chen HC, Wan HL, Chang DM. Ruptured renal microaneurysms complicated with a retroperitoneal abscess for a patient with systemic lupus erythematosus. Lupus. 2003; 12:317–320.9. Longstreth PL, Korobkin M, Palubinskas AJ. Renal microaneurysms in a patient with SLE. Radiology. 1974; 113:65–66.10. Stratton R, Bryce K, Beynon H, Tibballs J, Watkinson A, Davidson B. Systemic vasculitis with multiple aneurysms complicating systemic lupus erythematosus. J R Soc Med. 1999; 92:636–637.
Article11. Melamed N, Molad Y. Spontaneous retroperitoneal bleeding from renal microaneurysms and pancreatic pseudocyst in a patient with systemic lupus erythematosus. Scand J Rheumatol. 2006; 35:481–484.
Article12. Descombes E, Droz D, Drouet L, Grünfeld JP, Lesavre P. Renal vascular lesions in lupus nephritis. Medicine (Baltimore). 1997; 76:355–368.
Article13. Porcaro AB, Migliorini F, Pianon R, Antoniolli SZ, Furlan F, De Biase V, et al. Intraparenchymal renal artery aneurysms. Case report with review and update of the literature. Int Urol Nephrol. 2004; 36:409–416.
Article14. Koutoulidis V, Chatziioannou A, Kostopoulos C, Kontogiannis S, Skiadas V, Mourikis D, et al. Primary antiphospholipid syndrome: a unique presentation with multiple visceral aneurysms. Ann Rheum Dis. 2005; 64:1793–1794.
Article15. Dhaun N, Patel D, Kluth DC. Computed tomography angiography in the diagnosis of ANCA-associated small- and medium-vessel vasculitis. Am J Kidney Dis. 2013; 62:390–393.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multiple Dermatofibromas in a woman with Systemic Lupus Erythematosus
- Severe Hypophosphatemia in a Girl with Systemic Lupus Erythematosus
- A Case of Systemic Lupus Erythematosus Involving the Kidneys in a Patient with IgA Nephropathy
- Renal Artery Thrombosis in a Patient with Systemic Lupus Erythematosus without Antiphospholipid Antibody Syndrome: A Case Study
- A Case of Transverse Myelitis as a First Manifestation of Systemic Lupus Erythematosus
