Surgical Treatment of Chronic Tophaceous Gout in the 1st Metatarso-Phalangeal Joint
- Affiliations
-
- 1Department of Orthopedic Surgery, Pohang St. Mary's Hospital, Pohang, Korea. nammd60@hanmail.net
- KMID: 2428655
- DOI: http://doi.org/10.14193/jkfas.2018.22.4.156
Abstract
- PURPOSE
Chronic tophaceous gout is a painful and disabling inflammatory disease. Surgical treatment for chronic tophaceous gout is very difficult with many complications. This study evaluated the efficacy of shortening scarf osteotomy on the treatment of chronic tophaceous gout in the 1st metatarso-phalangeal (MTP) joint.
MATERIALS AND METHODS
From January 2006 to December 2015, 14 patients (19 cases) who underwent axial shortening scarf osteotomy for chronic tophaceous gout were reviewed. All patients were male. The average age at the time of surgery was 59.6 years (42~66 years). The minimum follow-up was 24 months. Total removal of the tophi mass with the adhered medial capsule of the 1st MTP joint was attempted. Axial shortening scarf osteotomy was done on the 1st metatarsal shaft. The visual analogue scale (VAS) for pain and the American Orthopaedic Foot and Ankle Society (AOFAS) forefoot score was assessed preoperatively and postoperatively. The range of motion (ROM) of the 1st MTP joint was also compared pre- and postoperatively.
RESULTS
The average size of the extracted tophaceous mass was 32 mm. The mean amount of the length of metatarsal shortening was 4.9 mm. The mean ROM of the 1st MTP joint was improved from 30.4° to 62.3°. The mean AOFAS forefoot score improved from 51.4 to 86.6 points. The mean VAS for pain improved from 4.6 to 0.3 points.
CONCLUSION
The axial shortening scarf osteotomy used on chronic tophaceous gout could reconstruct the 1st MTP joint with an improved ROM and was free of pain. Axial shortening scarf osteotomy is suggested as a useful and effective method for the treatment of chronic tophaceous gout.
Keyword
MeSH Terms
Figure
-

Figure 1. Preoperative radiograph (A) and clinical photograph (B).

Figure 2. (A, B) Removal of tophi mass with medial capsule of 1st metatarso-phalangeal (MTP) joint. (C) The status of articular cartilage of the 1st MTP joint was checked and the entire articular cartilage was covered by the chalky white materials.
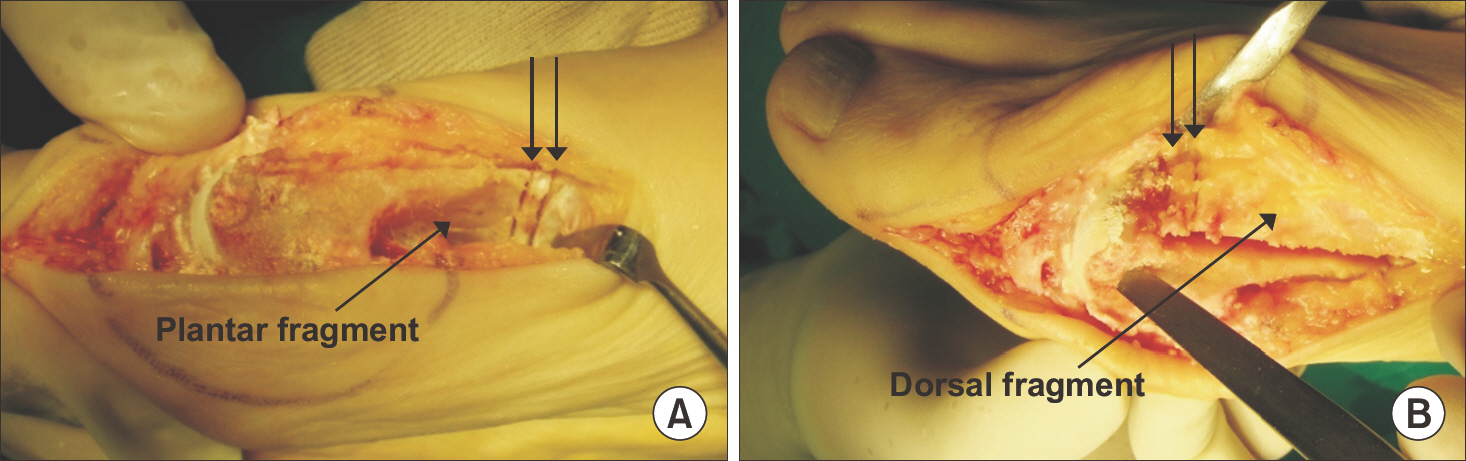
Figure 3. For shortening the 1st metatarsal, we cut the 1st metatarsal on both ends of scarf osteotomy fragments (plantar and dorsal fragments). (A) Plantar fragment. The distance between the two arrows shows the length of shortening. (B) Dorsal fragment. The distance between the two arrows shows the length of shortening.

Figure 4. After shortening scarf was done, we could achieve sufficient joint space (A; double-headed arrow) and improved range of motion of 1st metatarso-phalangeal joint compared to that of preoperative state. Passive dorsiflexion was improved after shortening at operation field (C) and follow-up (D) compared to that before shortening (B). Passive plantar flexion was improved after shortening at operation field (F) and follow-up (G) compared to that before shortening (E).

Figure 5. Radiograph (A) and clinical photograph (B) at 4-year followup.
Reference
-
1.Brook RA., Forsythe A., Smeeding JE., Lawrence Edwards N. Chronic gout: epidemiology, disease progression, treatment and disease burden. Curr Med Res Opin. 2010. 26:2813–21.
Article2.Poratt D., Rome K. Surgical Management of gout in the foot and ankle. A systematic review. J Am Podiatr Med Assoc. 2016. 106:182–8.3.Khanna D., Khanna PP., Fitzgerald JD., Singh MK., Bae S., Neogi T, et al. 2012 American College of Rheumatology guidelines for management of gout. Part 2: therapy and antiinflammatory prophylaxis of acute gouty arthritis. Arthritis Care Res (Hoboken). 2012. 64:1447–61.
Article4.Kemp TJ., Hirose CB., Coughlin MJ., Otto R. Treatment of chronic tophaceous gout with a wound vacuum-assisted device. Foot Ankle Int. 2010. 31:729–31.
Article5.Lin CT., Chang SC., Chen TM., Dai NT., Fu JP., Deng SC, et al. Free-flap resurfacing of tissue defects in the foot due to large gouty tophi. Microsurgery. 2011. 31:610–5.
Article6.Wünschel M., Wülker N., Walter C. Surgical treatment of a young patient with bilaterally destroyed first metatarsophalangeal joints suffering from gout. J Am Podiatr Med Assoc. 2012. 102:334–7.
Article7.Kim YS., Park EH., Lee HJ., Koh YG. First metatarsophalangeal joint arthrodesis for the treatment of tophaceous gouty arthritis. Orthopedics. 2014. 37:e141–7.
Article8.Wang CC., Lien SB., Huang GS., Pan RY., Shen HC., Kuo CL, et al. Arthroscopic elimination of monosodium urate deposition of the first metatarsophalangeal joint reduces the recurrence of gout. Arthroscopy. Arthroscopy. 2009. 25:153–8.
Article9.Barouk LS. Forefoot reconstruction. 2nd ed.Paris: Springer;2005. p. 305–12.10.Barouk LS., Barouk P. Joint-preserving surgery in rheumatoid forefoot: preliminary study with more-than-two-year followup. Foot Ankle Clin. 2007. 12:435–54. vi.
Article11.Coughlin MJ. Arthrodesis of the first metatarsophalangeal joint. Orthop Rev. 1990. 19:177–86.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Symptomatic Tophaceous Gout in the Bilateral Patellae
- Tophaceous Gout in the Rotator Cuff with Impingement Syndrome: A Case Report
- Acute Tophaceous Gout of the Distal Interphalangeal Joint Misdiagnosed as Cellulitis
- Irreducible Dorsal Dislocation of First Metatarsophalangeal Joint by Closed Method: Report of a Case
- Native 1st Metatarso-Phalangeal Joint Infection: A Rare Case Report
