Collagenous Spherulosis Associated with Lobular Carcinoma In Situ of the Breast: Two Case Reports
- Affiliations
-
- 1Department of Pathology, Chonnam National University Medical School, Gwangju, Korea. jshinlee@hanmail.net
- 2Department of Surgery, Chonnam National University Medical School, Gwangju, Korea.
- KMID: 2427526
- DOI: http://doi.org/10.4132/jptm.2018.03.29
Abstract
- No abstract available.
MeSH Terms
Figure
-
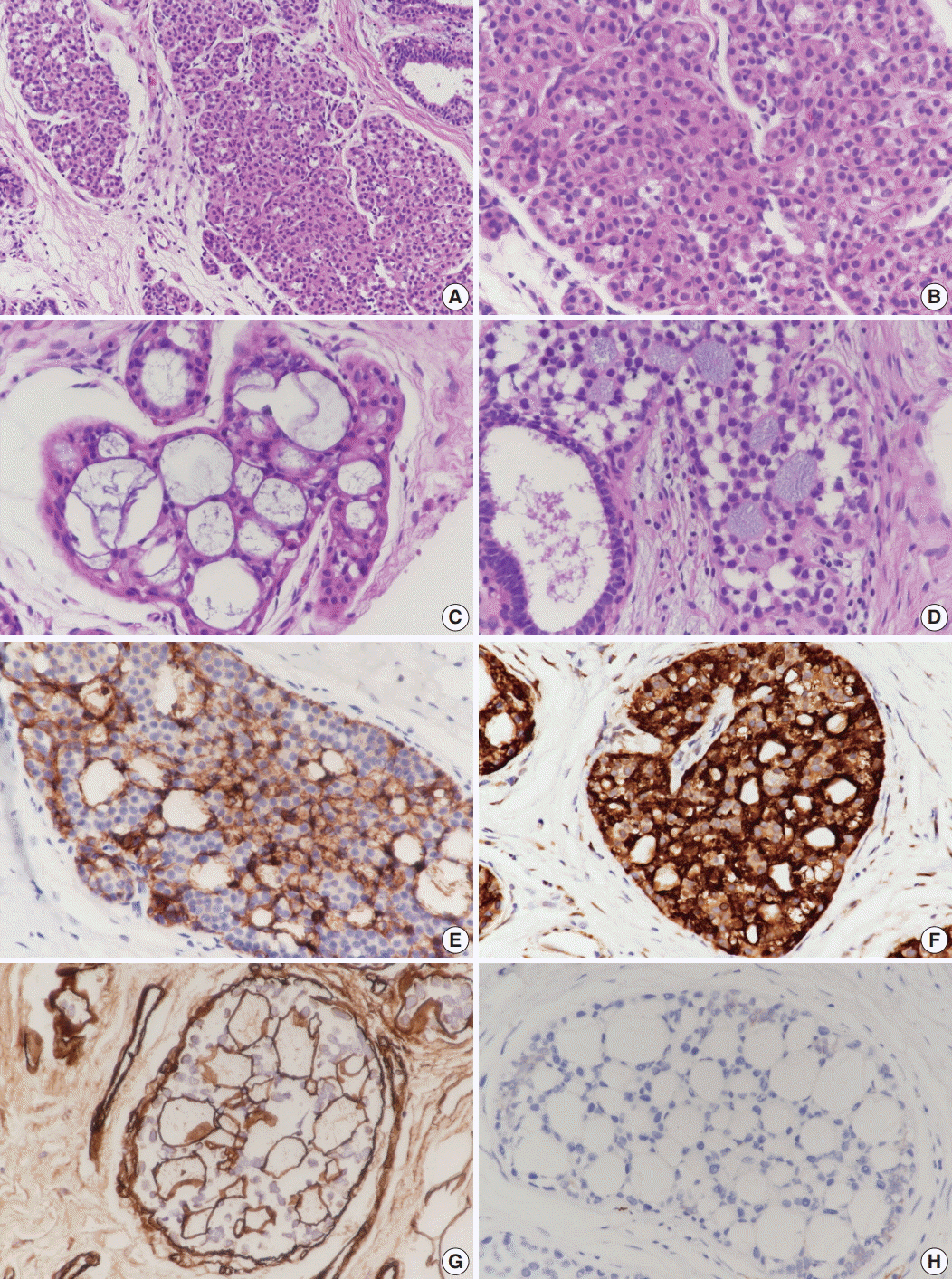
Fig. 1. Microscopic and immunohistochemical findings of case 1 collagenous spherulosis (CS) associated with lobular carcinoma in situ (LCIS), classical type. (A) In LCIS, enlarged lobules are seen. (B) The neoplastic cells of LCIS show loss of cohesion. (C) Cribriform proliferation with spherules containing cellular fibrillar components is seen. (D) LCIS cells colonize CS. (E) LCIS cells stain negative for E-cadherin, and the residual cells of CS stain positive. (F) Myoepithelial cells within CS with LCIS show calponin immunoreactivity. (G) Basement membrane-like components within spherules are highlighted by laminin immunostain. (H) CS with LCIS is negative for c-Kit.
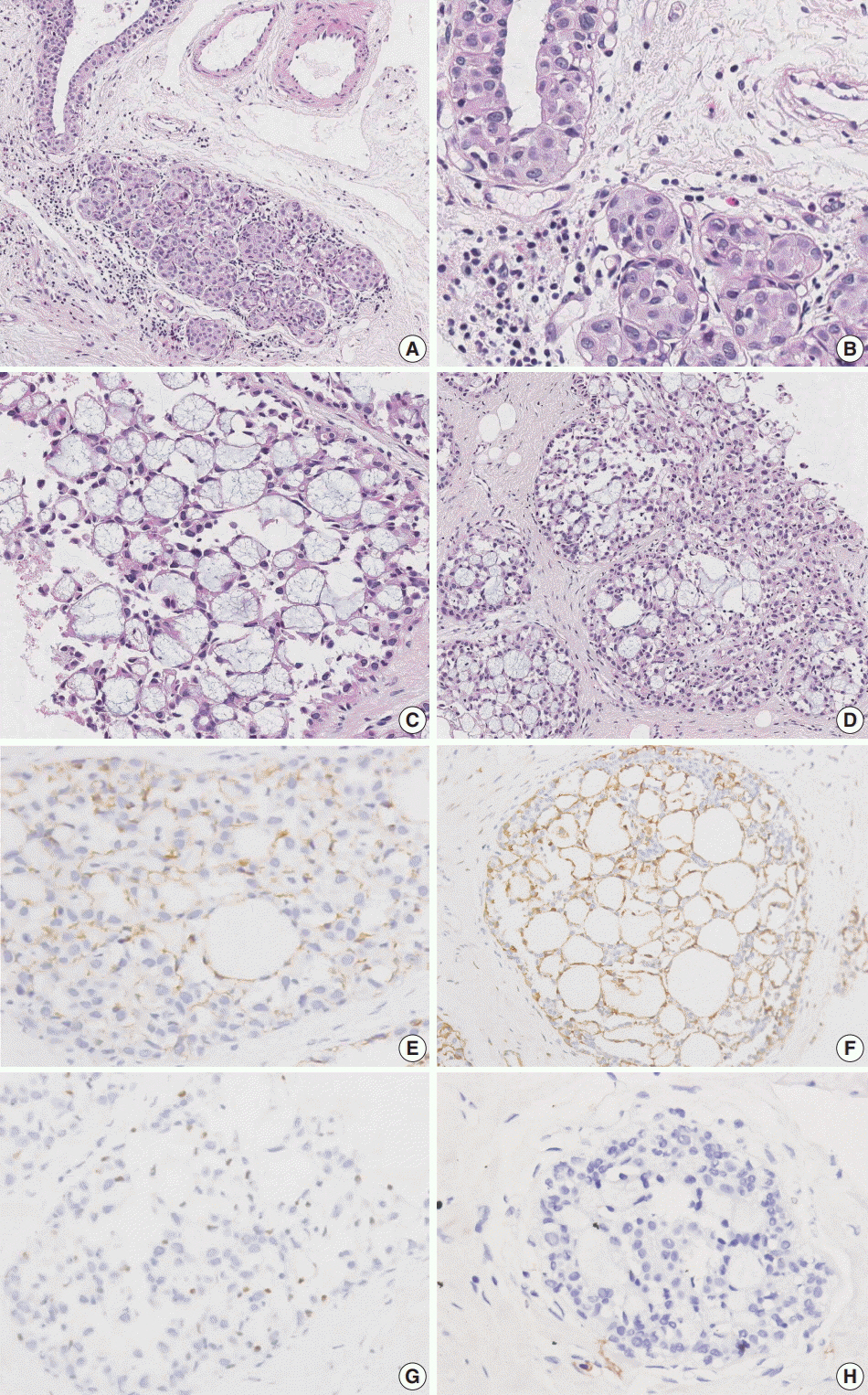
Fig. 2. Microscopic and immunohistochemical findings of case 2 collagenous spherulosis (CS) associated with lobular carcinoma in situ (LCIS), pleomorphic type. (A) The LCIS area shows enlarged lobular glands and intraepithelial growth pattern. (B) In contrast to case 1, the neoplastic cells contain more abundant cytoplasm and pleomorphic nuclei with occasional nucleoli. (C) A cribriform pattern of CS is characterized by cystic spaces containing basophilic fibrillar components. (D) CS with LCIS retains cribriform spaces, which contain cellular fibrillar components. (E) LCIS cells within the spherule show loss of E-cadherin expression. (F, G) The cells surrounding the spherules are positive for calpoinin and p63. (H) CS with LCIS is negative for c-Kit.
Reference
-
1. Clement PB, Young RH, Azzopardi JG. Collagenous spherulosis of the breast. Am J Surg Pathol. 1987; 11:411–7.
Article2. Mooney EE, Kayani N, Tavassoli FA. Spherulosis of the breast: a spectrum of municous and collagenous lesions. Arch Pathol Lab Med. 1999; 123:626–30.3. Resetkova E, Albarracin C, Sneige N. Collagenous spherulosis of breast: morphologic study of 59 cases and review of the literature. Am J Surg Pathol. 2006; 30:20–7.4. Hoda SA, Brogi E, Koerner FC, Rosen PP. Rosen’s breast pathology. 4th ed. Philadelphia: Lippincott Williams & Wilkins;2014. p. 143–7.5. Sgroi D, Koerner FC. Involvement of collagenous spherulosis by lobular carcinoma in situ: potential confusion with cribriform ductal carcinoma in situ. Am J Surg Pathol. 1995; 19:1366–70.
Article6. Eisenberg RE, Hoda SA. Lobular carcinoma in situ with collagenous spherulosis: clinicopathologic characteristics of 38 cases. Breast J. 2014; 20:440–1.
Article7. Toll A, Joneja U, Palazzo J. Pathologic spectrum of secretory and mucinous breast lesions. Arch Pathol Lab Med. 2016; 140:644–50.
Article8. Torous VF, Schnitt SJ, Collins LC. Benign breast lesions that mimic malignancy. Pathology. 2017; 49:181–96.
Article9. Cabibi D, Giannone AG, Belmonte B, Aragona F, Aragona F. CD10 and HHF35 actin in the differential diagnosis between Collagenous spherulosis and adenoid-cystic carcinoma of the breast. Pathol Res Pract. 2012; 208:405–9.
Article10. Rabban JT, Swain RS, Zaloudek CJ, Chase DR, Chen YY. Immunophenotypic overlap between adenoid cystic carcinoma and collagenous spherulosis of the breast: potential diagnostic pitfalls using myoepithelial markers. Mod Pathol. 2006; 19:1351–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Invasive Lobular Carcinoma of the Breast Associated with Mixed Lobular and Ductal Carcinoma In Situ: A Case Report
- Nodular Metastatic Carcinoma from Invasive Lobular Breast Cancer
- Lobular carcinoma in situ in sclerosing adenosis
- Multi-Focal Lobular Carcinoma In Situ Arising in Benign Phyllodes Tumor: A Case Report
- Signet Ring Cell Variant of Invasive Lobular Carcinoma of Male Breast
