Splenial Lesions of the Corpus Callosum: Disease Spectrum and MRI Findings
- Affiliations
-
- 1Department of Radiology, Gyeongsang National University School of Medicine, Jinju 52727, Korea. choids@gnu.ac.kr
- 2Gyeongsang Institute of Health Science, Gyeongsang National University School of Medicine, Jinju 52727, Korea.
- KMID: 2427240
- DOI: http://doi.org/10.3348/kjr.2017.18.4.710
Abstract
- The corpus callosum (CC) is the largest white matter structure in the brain, consisting of more than 200-250 million axons that provide a large connection mainly between homologous cerebral cortical areas in mirror image sites. The posterior end of the CC is the thickest part, which is called the splenium. Various diseases including congenital to acquired lesions including congenital anomalies, traumatic lesions, ischemic diseases, tumors, metabolic, toxic, degenerative, and demyelinating diseases, can involve the splenium of the CC and their clinical symptoms and signs are also variable. Therefore, knowledge of the disease entities and the imaging findings of lesions involving the splenium is valuable in clinical practice. MR imaging is useful for the detection and differential diagnosis of splenial lesions of the CC. In this study, we classify the disease entities and describe imaging findings of lesions involving the splenium of the CC based on our experiences and a review of the literature.
Keyword
MeSH Terms
Figure
-
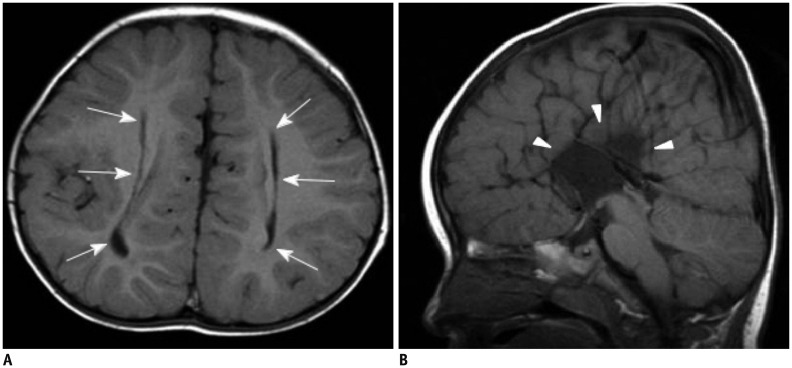
Fig. 1 1-year-old female patient with complete corpus callosal agenesis.A. T1-weighted axial image shows parallel configuration of both lateral ventricles (arrows). B. T1-weighted sagittal image reveals complete agenesis of corpus callosum (arrowheads).
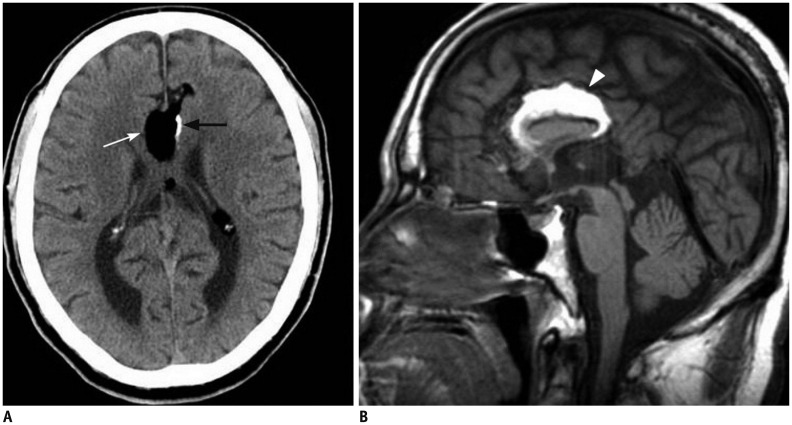
Fig. 2 70-year-old male patient with tubulonodular type pericallosal lipoma and partial corpus callosal agenesis.A. Axial CT image shows tubulonodular type lipoma in frontal interhemispheric fissure (white arrow). There is linear calcification at left side of lesion (black arrow). B. Sagittal T1-weighted MR image reveals partial agenesis of corpus callosum and hyperintense pericallosal lipoma (arrowhead).
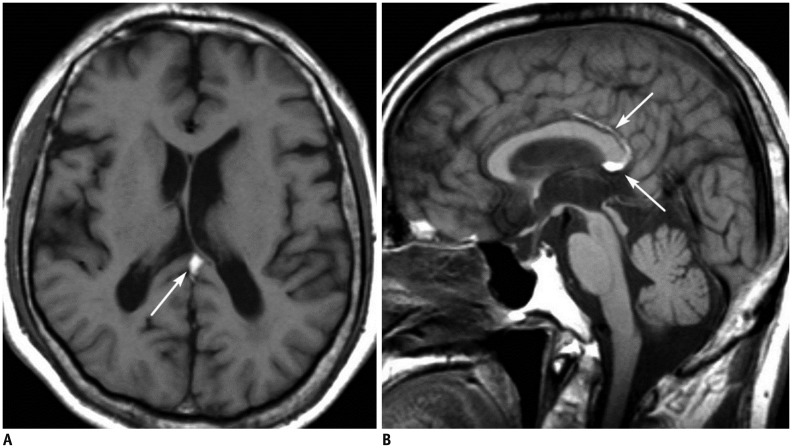
Fig. 3 64-year-old male patient with curvilinear type pericallosal lipoma and partial corpus callosal agenesis.T1-weighted axial (A) and sagittal (B) images show hyperintense lipoma (arrows) superior and posterior to corpus callosum. Splenial portion is not fully developed.
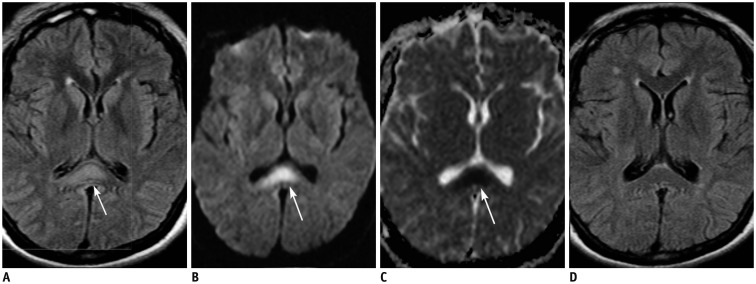
Fig. 4 29-year-old female patient with diffuse axonal injury lesion.Patient was involved in motor vehicle accident 9 days ago.A, B. Axial FLAIR (A) and DWI (B) images show hyperintense lesion in splenial portion of corpus callosum (arrows). Lesion is more conspicuously demonstrated on DWI than on FLAIR image. C. ADC map image reveals restricted water diffusion of lesion (arrow). D. On follow-up FLAIR image obtained 17 months later, splenial lesion has disappeared. ADC = apparent diffusion coeffcient, DWI = diffusion-weighted image, FLAIR = fluid-attenuated inversion recovery
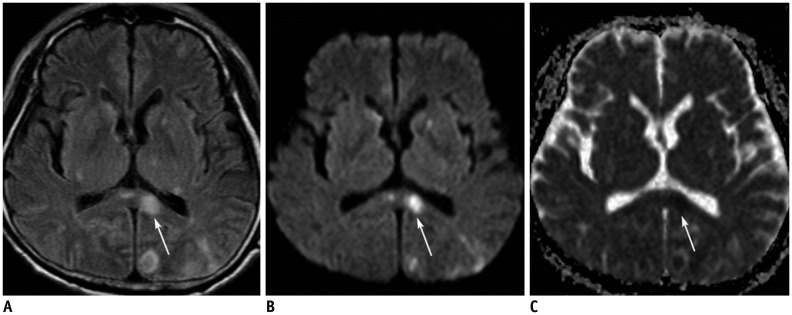
Fig. 5 62-year-old male patient with acute splenial infarction.A, B. Axial FLAIR image (A) and DWI (B) show multiple hyperintense lesions in bilateral basal ganglia, left thalamus, splenium of corpus callosum (arrows), and left occipital lobe. Splenial lesion (arrows) is more conspicuously demonstrated on DWI than on FLAIR image. C. ADC map image reveals restricted water diffusion of lesion (arrow). ADC = apparent diffusion coeffcient, DWI = diffusion-weighted image, FLAIR = fluid-attenuated inversion recovery
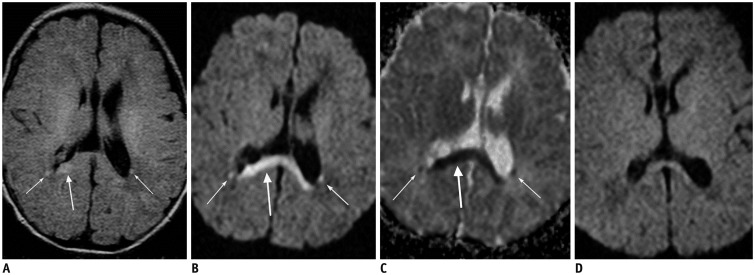
Fig. 6 8-day-old female patient with hypoxic-ischemic encephalopathy.Patient had birth asphyxia.A, B. Axial FLAIR image (A) and DWI (B) show hyperintense lesions in splenium of corpus callosum (thick arrows) and bilateral posterior deep periventricular white matter (thin arrows). C. ADC map image reveals restricted water diffusion of lesions (arrows). D. Follow-up axial DWI image obtained 1 month later shows decrease in signal intensity of lesions. ADC = apparent diffusion coeffcient, DWI = diffusion-weighted image, FLAIR = fluid-attenuated inversion recovery
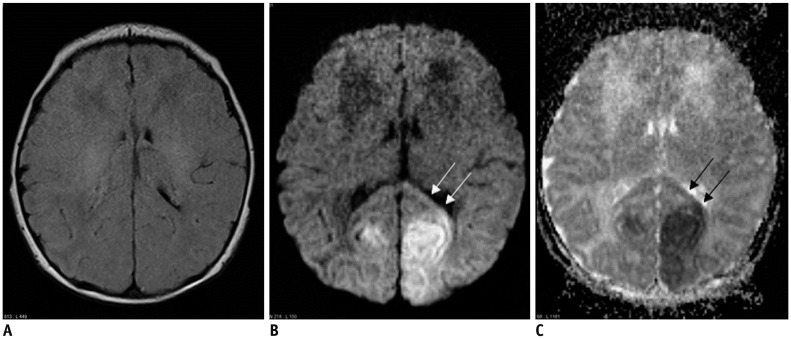
Fig. 7 2-day-old female with hypoglycemic encephalopathy.Glucose level was 2 mg/dL at presentation.A. On FLAIR axial image, there is no definite lesion. B. Axial DWI shows hyperintense lesions in both occipital lobes and splenium (arrows). C. ADC map image reveals restricted water diffusion of lesions (arrows). ADC = apparent diffusion coeffcient, DWI = diffusion-weighted image, FLAIR = fluid-attenuated inversion recovery
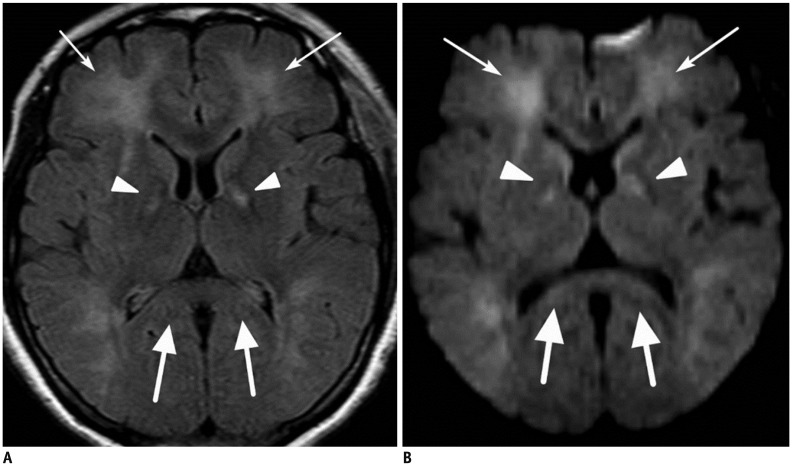
Fig. 8 48-year-old female patient with CO-intoxication.Axial FLAIR image (A) and DWI (B) show multiple hyperintense lesions in bilateral globus pallidus (arrowheads) and cerebral white matter (thin arrows) including splenium of corpus callosum (thick arrows). DWI = diffusion-weighted image, FLAIR = fluid-attenuated inversion recovery
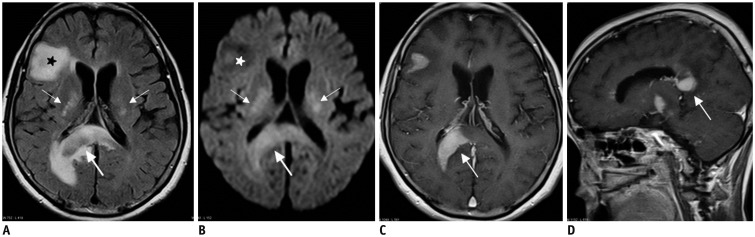
Fig. 9 61-year-old female patient with lymphomas.A, B. Axial FLAIR image (A) and DWI (B) show multiple hyperintense lesions in bilateral basal ganglia (thin arrows), splenium (thick arrows), and right frontal lobe (stars). C, D. On enhanced T1-weighted axial (C) and sagittal (D) images, splenial lesion (thick arrows) is homogeneously enhanced. DWI = diffusion-weighted image, FLAIR = fluid-attenuated inversion recovery
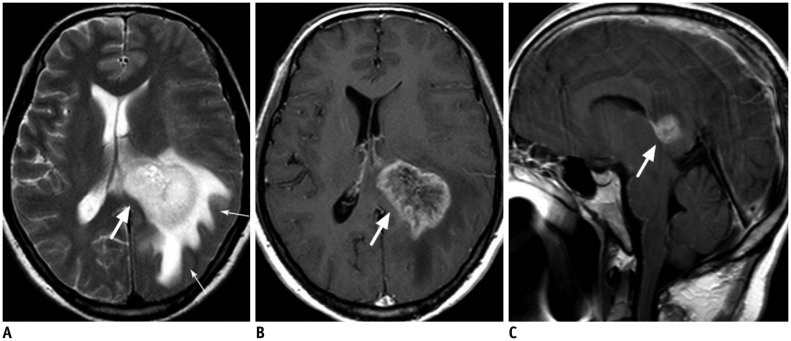
Fig. 10 52-year-old male patient with glioblastoma.A. Axial T2-weighted image shows large hyperintense mass in left deep periventricular white matter and adjacent splenium of corpus callosum (thick arrow). There is large amount of surrounding brain edema (thin arrows). B, C. On enhanced T1-weighted axial (B) and sagittal (C) images, mass is strongly enhanced (thick arrows).
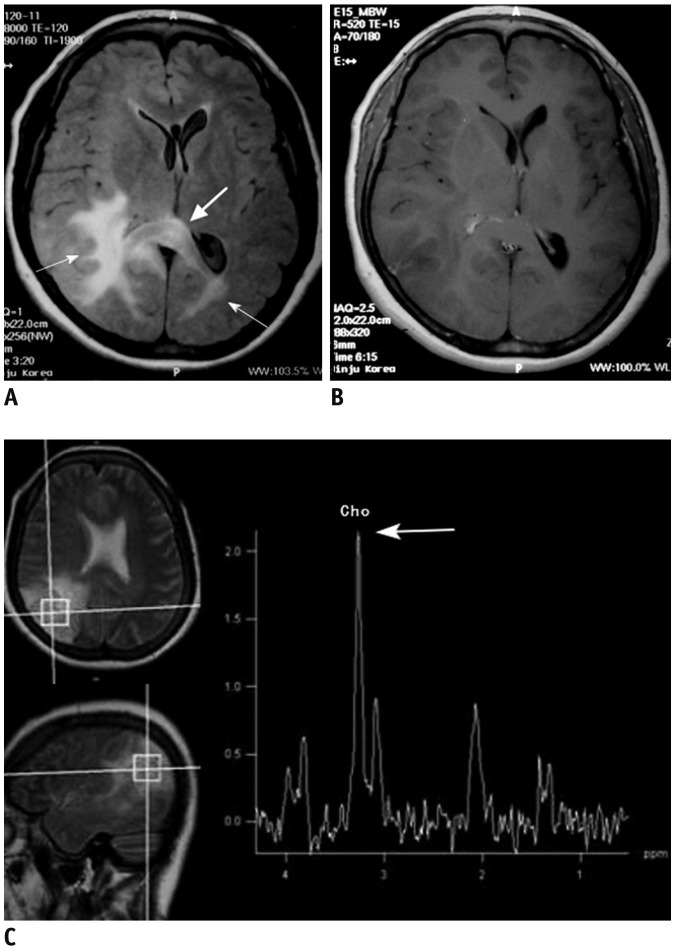
Fig. 11 46-year-old female patient with gliomatosis cerebri.A. Axial FLAIR image shows ill-defined hyperintense lesions involving bilateral posterior cerebral white matter (thin arrows) and splenium of corpus callosum (thick arrow). B. Enhanced T1-weighted axial image shows no definite contrast enhancement of lesion. C. Single voxel 1H MR spectroscopy reveals increased choline peak (thick arrow). FLAIR = fluid-attenuated inversion recovery

Fig. 12 32-year-old male patient with pineal germinoma.Enhanced T1-weighted sagittal image shows strong enhancing mass in pineal gland area. Mass extends into 3rd ventricle anteriorly and invades splenium of corpus callosum (arrow) and tectum inferiorly.
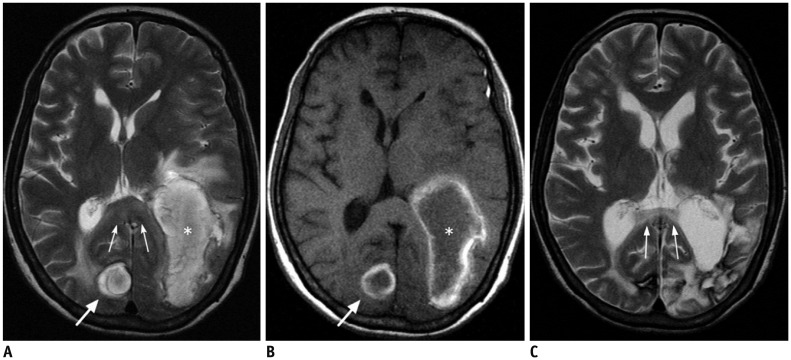
Fig. 13 49-year-old female patient with Wallerian degeneration due to intracerebral hematomas.A, B. Axial T2 (A) and T1-weighted (B) images show two hyperintense hematomas in right occipital lobe (thick arrows) and left temporooccipital lobes (asterisks). There is moderate amount of surrounding brain edema. Splenium also shows mild swelling and increased signal intensity (thin arrows). C. Follow-up T2-weighted image obtained 20 months later reveals atrophic change and increased signal intensity of splenium (thin arrows).
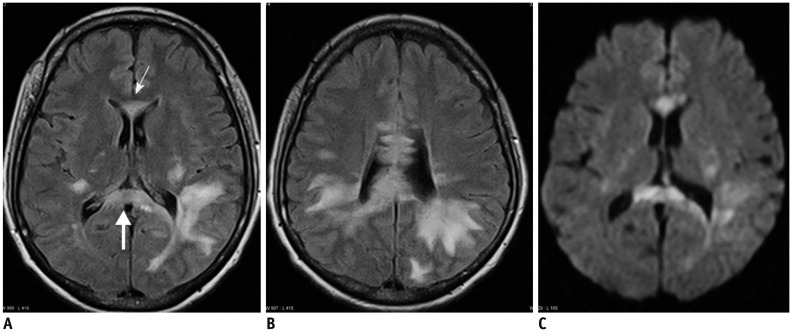
Fig. 14 39-year-old female patient with multiple sclerosis.A, B. Axial FLAIR images show multiple hyperintense lesions in both periventricular white matter, genu (thin arrow), and splenium (thick arrow) of corpus callosum. C. On DWI, most of lesions are demonstrated as hyperintensities. DWI = diffusion-weighted image, FLAIR = fluid-attenuated inversion recovery
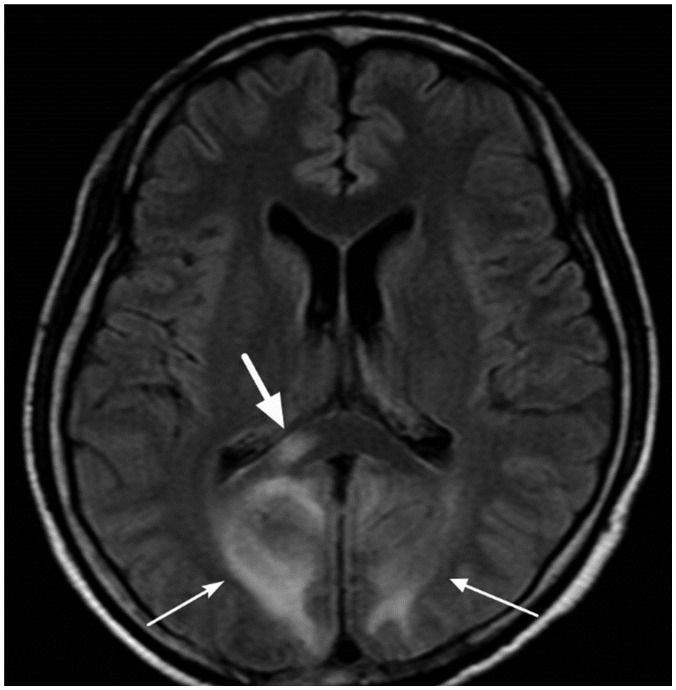
Fig. 15 29-year-old female patient with posterior reversible encephalopathy syndrome due to eclampsia.Axial FLAIR image shows multiple hyperintense lesions in cortices and white matter of both occipital lobes (thin arrows). There is also focal hyperintense lesion in right portion of splenium (thick arrow). FLAIR = fluid-attenuated inversion recovery
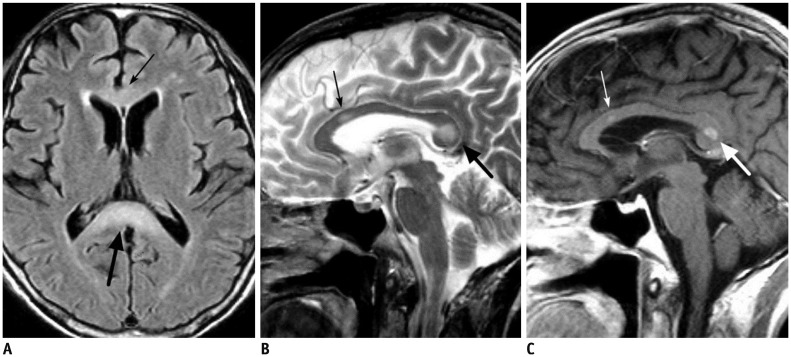
Fig. 16 59-year-old male patient with chronic alcoholism.A, B. FLAIR (A) and T2-weighted (B) images show hyperintense lesions in body (thin arrows) and splenial portion (thick arrows) of corpus callosum. C. There is focal contrast enhancement of lesions (arrows) on post-contrast T1-weighted image. FLAIR = fluid-attenuated inversion recovery
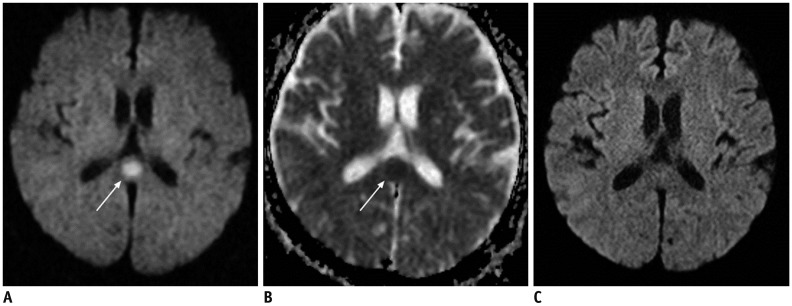
Fig. 17 62-year-old male patient with epilepsy.A. Axial DWI shows focal hyperintense lesion in splenium of corpus callosum (arrow). B. ADC map image reveals restricted water diffusion of lesion (arrow). C. On follow-up DWI obtained 14 days later, splenial lesion has disappeared. ADC = apparent diffusion coeffcient, DWI = diffusion-weighted image
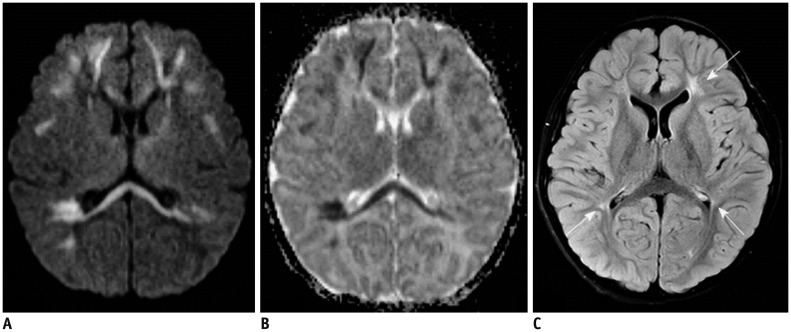
Fig. 18 5-day-old male with rotavirus-related white matter injury.A, B. Initial axial DWI (A) and ADC map (B) demonstrate extensive areas of restricted diffusion in periventricular white matter, deep white matter, corpus callosum, internal capsule, and posterior thalami. C. Follow-up FLAIR image obtained five years later shows residual ischemic lesions due to previous white matter injury in both periventricular white matters (arrows). ADC = apparent diffusion coeffcient, DWI = diffusion-weighted image, FLAIR = fluid-attenuated inversion recovery
Reference
-
1. Lee SK, Kim DI, Kim J, Kim DJ, Kim HD, Kim DS, et al. Diffusion-tensor MR imaging and fiber tractography: a new method of describing aberrant fiber connections in developmental CNS anomalies. Radiographics. 2005; 25:53–65. discussion 66-68. PMID: 15653586.
Article2. Doherty MJ, Jayadev S, Watson NF, Konchada RS, Hallam DK. Clinical implications of splenium magnetic resonance imaging signal changes. Arch Neurol. 2005; 62:433–437. PMID: 15767508.
Article3. Park MK, Hwang SH, Jung S, Hong SS, Kwon SB. Lesions in the splenium of the corpus callosum: clinical and radiological implications. Neurol Asia. 2014; 19:79–88.4. Li S, Sun X, Bai YM, Qin HM, Wu XM, Zhang X, et al. Infarction of the corpus callosum: a retrospective clinical investigation. PLoS One. 2015; 10:e0120409. PMID: 25785450.
Article5. Georgy BA, Hesselink JR, Jernigan TL. MR imaging of the corpus callosum. AJR Am J Roentgenol. 1993; 160:949–955. PMID: 8470609.
Article6. Barkovich AJ, Norman D. Anomalies of the corpus callosum: correlation with further anomalies of the brain. AJR Am J Roentgenol. 1988; 151:171–179. PMID: 3259802.
Article7. Truwit CL, Barkovich AJ. Pathogenesis of intracranial lipoma: an MR study in 42 patients. AJR Am J Roentgenol. 1990; 155:855–864. discussion 865. PMID: 2119122.
Article8. Ginat DT, Meyers SP. Intracranial lesions with high signal intensity on T1-weighted MR images: differential diagnosis. Radiographics. 2012; 32:499–516. PMID: 22411945.
Article9. Uchino A, Takase Y, Nomiyama K, Egashira R, Kudo S. Acquired lesions of the corpus callosum: MR imaging. Eur Radiol. 2006; 16:905–914. PMID: 16284771.
Article10. Provenzale JM. Imaging of traumatic brain injury: a review of the recent medical literature. AJR Am J Roentgenol. 2010; 194:16–19. PMID: 20028899.
Article11. Arfanakis K, Haughton VM, Carew JD, Rogers BP, Dempsey RJ, Meyerand ME. Diffusion tensor MR imaging in diffuse axonal injury. AJNR Am J Neuroradiol. 2002; 23:794–802. PMID: 12006280.12. Scheid R, Preul C, Gruber O, Wiggins C, von Cramon DY. Diffuse axonal injury associated with chronic traumatic brain injury: evidence from T2*-weighted gradient-echo imaging at 3 T. AJNR Am J Neuroradiol. 2003; 24:1049–1056. PMID: 12812926.13. Chrysikopoulos H, Andreou J, Roussakis A, Pappas J. Infarction of the corpus callosum: computed tomography and magnetic resonance imaging. Eur J Radiol. 1997; 25:2–8. PMID: 9248790.
Article14. Kasow DL, Destian S, Braun C, Quintas JC, Kagetsu NJ, Johnson CE. Corpus callosum infarcts with atypical clinical and radiologic presentations. AJNR Am J Neuroradiol. 2000; 21:1876–1880. PMID: 11110540.15. Ho ML, Moonis G, Ginat DT, Eisenberg RL. Lesions of the corpus callosum. AJR Am J Roentgenol. 2013; 200:W1–W16. PMID: 23255767.
Article16. Chao CP, Zaleski CG, Patton AC. Neonatal hypoxic-ischemic encephalopathy: multimodality imaging findings. Radiographics. 2006; 26(Suppl 1):S159–S172. PMID: 17050513.
Article18. Kang EG, Jeon SJ, Choi SS, Song CJ, Yu IK. Diffusion MR imaging of hypoglycemic encephalopathy. AJNR Am J Neuroradiol. 2010; 31:559–564. PMID: 19875472.
Article19. Beltran-Marin M, Sadeghi N. Transient restricted diffusion in the splenium of the corpus callosum after brain surgery. JBR-BT. 2013; 96:92.
Article20. Lo CP, Chen SY, Lee KW, Chen WL, Chen CY, Hsueh CJ, et al. Brain injury after acute carbon monoxide poisoning: early and late complications. AJR Am J Roentgenol. 2007; 189:W205–W211. PMID: 17885032.
Article21. Beppu T. The role of MR imaging in assessment of brain damage from carbon monoxide poisoning: a review of the literature. AJNR Am J Neuroradiol. 2014; 35:625–631. PMID: 23598831.
Article22. Bourekas EC, Varakis K, Bruns D, Christoforidis GA, Baujan M, Slone HW, et al. Lesions of the corpus callosum: MR imaging and differential considerations in adults and children. AJR Am J Roentgenol. 2002; 179:251–257. PMID: 12076946.
Article23. Kim M, Kim HS. Emerging techniques in brain tumor imaging: what radiologists need to know. Korean J Radiol. 2016; 17:598–619. PMID: 27587949.
Article24. Gupta RK, Saksena S, Hasan KM, Agarwal A, Haris M, Pandey CM, et al. Focal Wallerian degeneration of the corpus callosum in large middle cerebral artery stroke: serial diffusion tensor imaging. J Magn Reson Imaging. 2006; 24:549–555. PMID: 16888796.
Article25. Brass SD, Caramanos Z, Santos C, Dilenge ME, Lapierre Y, Rosenblatt B. Multiple sclerosis vs acute disseminated encephalomyelitis in childhood. Pediatr Neurol. 2003; 29:227–231. PMID: 14629906.
Article26. Bartynski WS, Boardman JF. Distinct imaging patterns and lesion distribution in posterior reversible encephalopathy syndrome. AJNR Am J Neuroradiol. 2007; 28:1320–1327. PMID: 17698535.
Article27. Arbelaez A, Pajon A, Castillo M. Acute Marchiafava-Bignami disease: MR findings in two patients. AJNR Am J Neuroradiol. 2003; 24:1955–1957. PMID: 14625216.28. Kim E, Na DG, Kim EY, Kim JH, Son KR, Chang KH. MR imaging of metronidazole-induced encephalopathy: lesion distribution and diffusion-weighted imaging findings. AJNR Am J Neuroradiol. 2007; 28:1652–1658. PMID: 17885234.
Article29. Hirotani M, Yabe I, Hamada S, Tsuji S, Kikuchi S, Sasaki H. Abnormal brain MRI signals in the splenium of the corpus callosum, basal ganglia and internal capsule in a suspected case with tuberculous meningitis. Intern Med. 2007; 46:505–509. PMID: 17443044.
Article30. Conti M, Salis A, Urigo C, Canalis L, Frau S, Canalis GC. Transient focal lesion in the splenium of the corpus callosum: MR imaging with an attempt to clinical-physiopathological explanation and review of the literature. Radiol Med. 2007; 112:921–935. PMID: 17885738.
Article31. Malhotra HS, Garg RK, Vidhate MR, Sharma PK. Boomerang sign: clinical significance of transient lesion in splenium of corpus callosum. Ann Indian Acad Neurol. 2012; 15:151–157. PMID: 22566735.
Article32. Yeom JS, Kim YS, Seo JH, Park JS, Park ES, Lim JY, et al. Distinctive pattern of white matter injury in neonates with rotavirus infection. Neurology. 2015; 84:21–27. PMID: 25471392.
Article33. Amarnath C, Helen Mary T, Periakarupan A, Gopinathan K, Philson J. Neonatal parechovirus leucoencephalitis-radiological pattern mimicking hypoxic-ischemic encephalopathy. Eur J Radiol. 2016; 85:428–434. PMID: 26781149.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Transient Splenial Lesion of the Corpus Callosum in Patients with Infectious Disease
- A Case of Transient Isolated Splenial Lesion of the Corpus Callosum After New Onset Seizure
- Reversible Splenial Lesion in the Corpus Callosum on MRI after Ingestion of a Herbicide Containing Glufosinate Ammonium: A Case Report
- Transient splenial lesions of the corpus callosum and infectious diseases
- Agenesis of Corpus Callosum
