Ann Surg Treat Res.
2018 Dec;95(6):340-344. 10.4174/astr.2018.95.6.340.
Traumatic lumbar hernia: clinical features and management
- Affiliations
-
- 1Department of Trauma, Gachon University Gil Medical Center, Incheon, Korea. yepark26@gmail.com
- KMID: 2426766
- DOI: http://doi.org/10.4174/astr.2018.95.6.340
Abstract
- PURPOSE
Traumatic lumbar hernia is rare, thus making diagnosis and proper treatment challenging. Accordingly, we aimed to investigate the clinical manifestations and proper management strategies of traumatic lumbar hernias.
METHODS
The medical records of patients with traumatic lumbar hernia treated at Gachon University Gil Hospital from March 2006 to February 2015, were retrospectively reviewed.
RESULTS
We included 5 men and 4 women (mean age, 55 years; range, 23-71 years). In 8 patients, most injuries were caused by motor vehicle collisions, including those wherein a pedestrian was struck (5 cases of car accidents, 2 falls, and 1 involving penetrating materials); in 1 patient, the probable cause was severe cough. Eight patients underwent hernia repair surgery (5 open and 3 laparoscopic), and a prosthetic mesh was used in 7 patients. Hernia repairs were elective in 7 patients; emergency hernia repair was performed with right hemicolectomy in 1 patient. No severe complication or recurrence was observed. Only 2 patients had mild complications, such as postoperative seroma.
CONCLUSION
Traumatic lumbar hernia is a relatively rare injury of the posteriolateral abdominal wall. Lumbar hernia should be suspected in patients with high-energy injuries of the torso, and all such patients should undergo abdominopelvic computed tomography. After diagnosis, hernia repair can be electively performed without complications in most cases.
Keyword
MeSH Terms
Figure
-
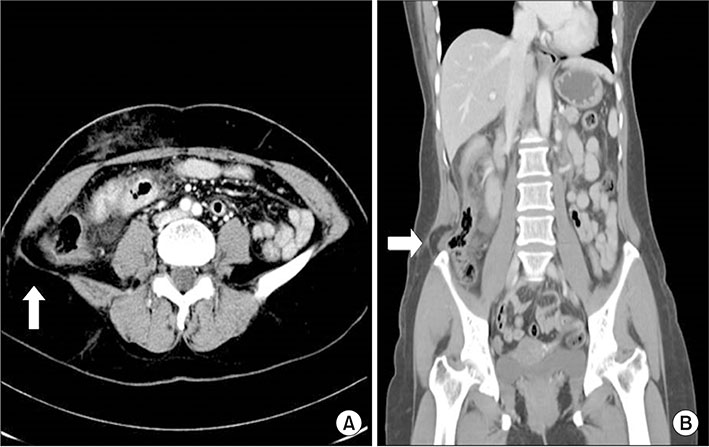
Fig. 1 Abdominopelvic CT scan (A: axial view, B: coronal view) shows the lumbar area wall defect (arrows).
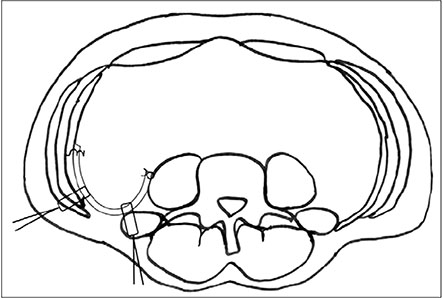
Fig. 2 Mesh fixation. Transfascial fixations are used to fix mesh around the margin of the defect. The periphery of mesh is fixed to the abdominal wall with tacks and to the psoas muscle with sutures.

Fig. 3 Total extraperitoneal approach was used for laparoscopic hernia repair. Arrows indicate lumbar wall defect in the extraperitoneal space. Arrowheads indicate preperitoneal fat in the hernia site.
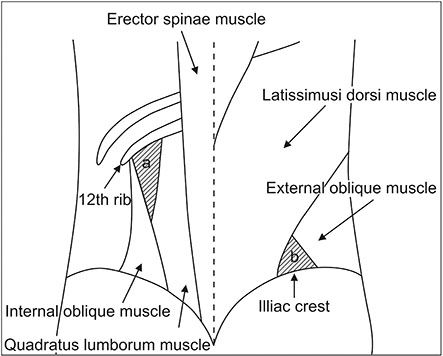
Fig. 4 Anatomic locations of lumbar hernias. (a) Superior lumbar hernia (Grynfeltt-Lesshaft triangle). (b) Inferior lumbar hernia (Petit triangle).
Reference
-
1. Moreno-Egea A, Baena EG, Calle MC, Martinez JA, Albasini JL. Controversies in the current management of lumbar hernias. Arch Surg. 2007; 142:82–88.
Article2. Burt BM, Afifi HY, Wantz GE, Barie PS. Traumatic lumbar hernia: report of cases and comprehensive review of the literature. J Trauma. 2004; 57:1361–1370.
Article3. Geis WP, Saletta JD. Lumbar hernia. In : Nyhus LM, Condon RE, editors. Hernia. Philadelphia (PA): Lippincott;1989. p. 401–415.4. Zhou X, Nve JO, Chen G. Lumbar hernia: clinical analysis of 11 cases. Hernia. 2004; 8:260–263.
Article5. Presti JC Jr, Narayan P. Lumbar herniation of the kidney. J Urol. 1988; 140:586–587.
Article6. Shuhaiber J, Dunn T, Evans A, Fishman D, Merlotti G, Salzman S. Traumatic lumbar hernia with ureteropelvic junction disruption: case report and review of the literature. J Trauma. 2003; 55:985–988.
Article7. Biotois H, Couinaud C. A case of lumbar hernia favoring the formation of a mass in the pelvic colon. J Chir (Paris). 1969; 98:27–30.8. Lauritzen JB, Ebbehoj N. Retropancreatic abscess. Intermittent lumbar hernia. Ugeskr Laeger. 1985; 147:526.9. Zub A, Kozka M. Petit's triangle hernia clinically mimicking gluteal abscess. Przegl Lek. 2003; 60:Suppl 7. 86–87.10. Skrekas G, Stafyla VK, Papalois VE. A Grynfeltt hernia: report of a case. Hernia. 2005; 9:188–191.
Article11. Arca MJ, Heniford BT, Pokorny R, Wilson MA, Mayes J, Gagner M. Laparoscopic repair of lumbar hernias. J Am Coll Surg. 1998; 187:147–152.
Article12. Bickel A, Haj M, Eitan A. Laparoscopic management of lumbar hernia. Surg Endosc. 1997; 11:1129–1130.
Article13. Moreno-Egea A, Torralba-Martinez JA, Morales G, Fernandez T, Girela E, Aguayo-Albasini JL. Open vs laparoscopic repair of secondary lumbar hernias: a prospective nonrandomized study. Surg Endosc. 2005; 19:184–187.
Article14. Heniford BT, Iannitti DA, Gagner M. Laparoscopic inferior and superior lumbar hernia repair. Arch Surg. 1997; 132:1141–1144.
Article15. Shekarriz B, Graziottin TM, Gholami S, Lu HF, Yamada H, Duh QY, et al. Transperitoneal preperitoneal laparoscopic lumbar incisional herniorrhaphy. J Urol. 2001; 166:1267–1269.
Article16. Meinke AK. Totally extraperitoneal laparoendoscopic repair of lumbar hernia. Surg Endosc. 2003; 17:734–737.
Article17. Postema RR, Bonjer HJ. Endoscopic extraperitoneal repair of a Grynfeltt hernia. Surg Endosc. 2002; 16:716.
Article18. Habib E. Retroperitoneoscopic tension-free repair of lumbar hernia. Hernia. 2003; 7:150–152.
Article19. Moreno-Egea A, Aguayo JL. Ambulatory laparoscopic repair of inferior lumbar or Petit hernia: a case report. Surg Endosc. 2002; 16:1107.20. Salameh JR, Salloum EJ. Lumbar incisional hernias: diagnostic and management dilemma. JSLS. 2004; 8:391–394.21. Killeen KL, Girard S, DeMeo JH, Shanmuganathan K, Mirvis SE. Using CT to diagnose traumatic lumbar hernia. AJR Am J Roentgenol. 2000; 174:1413–1415.
Article
