Investig Clin Urol.
2016 May;57(3):221-228. 10.4111/icu.2016.57.3.221.
Robot-assisted partial cystectomy with intraoperative frozen section examination: Evolution and evaluation of a novel technique
- Affiliations
-
- 1Vattikuti Urology Institute, Henry Ford Health System, Detroit, MI, USA. asood1@hfhs.org
- KMID: 2426498
- DOI: http://doi.org/10.4111/icu.2016.57.3.221
Abstract
- PURPOSE
To describe a novel modification to robot-assisted partial cystectomy (RAPC) that allows for intraoperative surgical margin assessment by bimanual-examination and frozen-section analysis.
MATERIALS AND METHODS
A total of 7 patients underwent RAPC at a single tertiary-care institution between 2008 and 2013. The technique evolved over the study-period and permitted real-time intraoperative surgical margin evaluation in the last 5 patients via bimanual-examination and frozen-section analysis, utilizing the GelPOINT platform (a hand-assist device). The GelPOINT platform was placed through a 4- to 5-cm vertical supraumbilical incision and allowed for rapid retrieval of the bladder specimen without compromising the pneumoperitoneum or prolonging the operative time. Perioperative, oncological and functional outcomes were evaluated; all patients had a minimum 12-month follow-up. At the time of last follow-up, a cross-sectional survey of patients was performed to evaluate regret/satisfaction utilizing validated questionnaires.
RESULTS
The mean age was 72.5 years; 71.4% of the patients were men (n=5). All patients underwent RAPC for a malignant indication. The mean operative and console times were 291 and 217 minutes, respectively. No patient had a positive surgical margin. Mean length-of-stay was 1.7 days. At a median follow-up of 38.9 months, 1 patient experienced a local recurrence 6 months postsurgery. The only mortality was secondary to Lewy-body disease, in the same patient, 1 year postoperatively. Patient assessment of regret and satisfaction indicated 0% regret and 0% dissatisfaction.
CONCLUSIONS
The 'modified' technique of RAPC is technically feasible, safe, and reproducible; further, RAPC leads to favorable oncological, functional and quality-of-life outcomes in patients eligible for partial cystectomy.
MeSH Terms
-
Aged
Cystectomy/adverse effects/*methods/rehabilitation
Female
Follow-Up Studies
*Frozen Sections
Humans
Intraoperative Care/*methods
Male
Margins of Excision
Middle Aged
Operative Time
Patient Satisfaction
Quality of Life
Robotic Surgical Procedures/adverse effects/*methods/rehabilitation
Specimen Handling/methods
Ultrasonography
Urinary Bladder Neoplasms/diagnostic imaging/pathology/*surgery
Figure
-
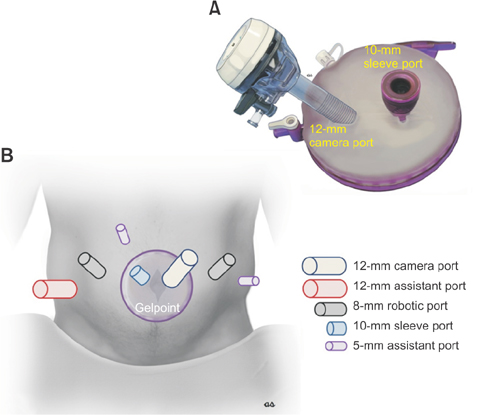
Fig. 1 (A) GelSeal cap prepared with the 12-mm camera port and 10-mm sleeve port. (B) Port placement for robot-assisted partial cystectomy.
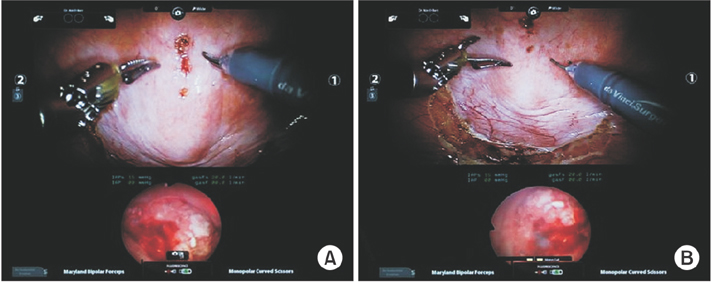
Fig. 2 (A, B) Concurrent cystoscopic and robotic view for accurate tumor demarcation.
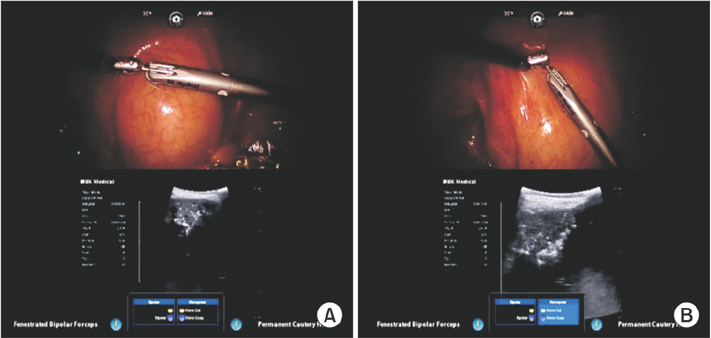
Fig. 3 (A, B) Ultrasound confirmation of tumor location using the drop-down robotic ultrasound probe.

Fig. 4 (A-E) Progressive circumferential scoring of the peritoneal aspect of the bladder around the tumor with a 10- to 20-mm margin.
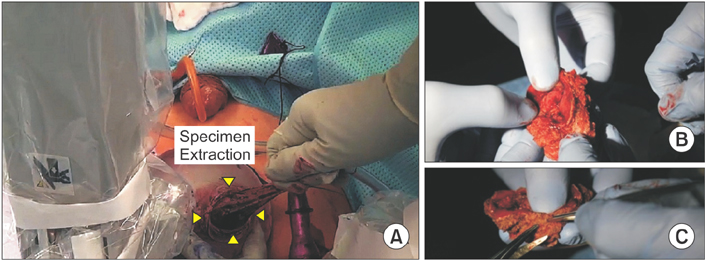
Fig. 5 (A) Extracting the partial cystectomy specimen for bimanual and frozen-section assessment. (B, C) Bimanual examination and frozen-section analysis.
Reference
-
1. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013; 63:11–30.2. Vaidya A, Soloway MS, Hawke C, Tiguert R, Civantos F. De novo muscle invasive bladder cancer: is there a change in trend? J Urol. 2001; 165:47–50.3. Ghoneim MA, el-Mekresh MM, el-Baz MA, el-Attar IA, Ashamallah A. Radical cystectomy for carcinoma of the bladder: critical evaluation of the results in 1,026 cases. J Urol. 1997; 158:393–399.4. Kassouf W, Swanson D, Kamat AM, Leibovici D, Siefker-Radtke A, Munsell MF, et al. Partial cystectomy for muscle invasive urothelial carcinoma of the bladder: a contemporary review of the M. D. Anderson Cancer Center experience. J Urol. 2006; 175:2058–2062.5. Ferzli G, Wenof M, Giannakakos A, Raboy A, Albert P. Laparoscopic partial cystectomy for vesical endometrioma. J Laparoendosc Surg. 1993; 3:161–165.6. Mariano MB, Tefilli MV. Laparoscopic partial cystectomy in bladder cancer: initial experience. Int Braz J Urol. 2004; 30:192–198.7. Colombo Jr JR, Desai M, Canes D, Frota R, Haber GP, Moinzadeh A, et al. Laparoscopic partial cystectomy for urachal and bladder cancer. Clinics (Sao Paulo). 2008; 63:731–734.8. Tareen BU, Mufarrij PW, Godoy G, Stifelman MD. Robot-assisted laparoscopic partial cystectomy and diverticulectomy: initial experience of four cases. J Endourol. 2008; 22:1497–1500.9. Allaparthi S, Ramanathan R, Balaji KC. Robotic partial cystectomy for bladder cancer: a single-institutional pilot study. J Endourol. 2010; 24:223–227.10. Jeong W, Sood A, Ghani KR, Pucheril D, Sammon JD, Gupta NS, et al. Bimanual examination of the retrieved specimen and regional hypothermia during robot-assisted radical prostatectomy: a novel technique for reducing positive surgical margin and achieving pelvic cooling. BJU Int. 2014; 114:955–957.11. Rogers CG, Ghani KR, Kumar RK, Jeong W, Menon M. Robotic partial nephrectomy with cold ischemia and on-clamp tumor extraction: recapitulating the open approach. Eur Urol. 2013; 63:573–578.12. Mostofi FK, Davis CJ, Sesterhenn IA, Sobin LH. Histological typing of urinary bladder tumours. Berlin: Springer;1999.13. Clark JA, Wray NP, Ashton CM. Living with treatment decisions: regrets and quality of life among men treated for metastatic prostate cancer. J Clin Oncol. 2001; 19:72–80.14. Schroeck FR, Krupski TL, Sun L, Albala DM, Price MM, Polascik TJ, et al. Satisfaction and regret after open retropubic or robot-assisted laparoscopic radical prostatectomy. Eur Urol. 2008; 54:785–793.15. Menon M, Hemal AK, Tewari A, Shrivastava A, Shoma AM, El-Tabey NA, et al. Nerve-sparing robot-assisted radical cystoprostatectomy and urinary diversion. BJU Int. 2003; 92:232–236.16. Ashley RA, Inman BA, Sebo TJ, Leibovich BC, Blute ML, Kwon ED, et al. Urachal carcinoma: clinicopathologic features and long-term outcomes of an aggressive malignancy. Cancer. 2006; 107:712–720.17. Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst. 1959; 22:719–748.18. Brickman P, Coates D, Janoff-Bulman R. Lottery winners and accident victims: is happiness relative? J Pers Soc Psychol. 1978; 36:917–927.19. Menon M, Abaza R, Sood A, Ahlawat R, Ghani KR, Jeong W, et al. Robotic kidney transplantation with regional hypothermia: evolution of a novel procedure utilizing the IDEAL guidelines (IDEAL phase 0 and 1). Eur Urol. 2014; 65:1001–1009.20. McCulloch P, Altman DG, Campbell WB, Flum DR, Glasziou P, Marshall JC, et al. No surgical innovation without evaluation: the IDEAL recommendations. Lancet. 2009; 374:1105–1112.21. Barkun JS, Aronson JK, Feldman LS, Maddern GJ, Strasberg SM, et al. Balliol Collaboration. Evaluation and stages of surgical innovations. Lancet. 2009; 374:1089–1096.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Technique of Partial Cystectomy for Carcinoma
- The Value of Routine Frozen Section Examination for Intraoperative Diagnosis of Thyroid Nodule
- The Accuracy of Frozen Section Diagnosis of Gynecologic Tumors
- The Role of Fine-Needle Aspiration Cytology and Frozen Section in the Operative Management of Thyroid Nodule
- Intraoperative consultation for ovarian tumors
