Computed Tomography Enterography for Evaluation of Inflammatory Bowel Disease
- Affiliations
-
- 1Department of Radiology, Yonsei University Health System, Yonsei University College of Medicine, Seoul, Korea. jslim1@yuhs.ac
Abstract
- Computed tomography enterography (CTE) has become a main modality for the evaluation of inflammatory bowel disease (IBD). It simultaneously offers visualization of the small bowel and extraintestinal status, which is helpful for diagnosing IBD. Crohn disease has long segmental enhancing wall thickening related with the eccentric longitudinal distribution. In addition, mural stratification, fibrofatty proliferation, positive comb sign by increased mesenteric vascularity and internal/perianal fistula are characteristics of Crohn disease and can be identified on CTE. Short segmental inflammatory wall thickening and the central low attenuated lymph nodes are favorable CT finding of intestinal tuberculosis. A geographic, relatively large, and deep penetrating ulcer with bowel wall thickening and mural hyperenhancement in ileocecal area are characteristics of intestinal Behcet disease. Each of CTE findings for the IBDs is helpful for differential diagnosis. The main disadvantage of this technique is the requisite radiation exposure of patients, particularly in young patients. However, recent development of advanced CT techniques is promising for radiation dose reduction without compromising diagnostic image quality.
Keyword
MeSH Terms
Figure
-
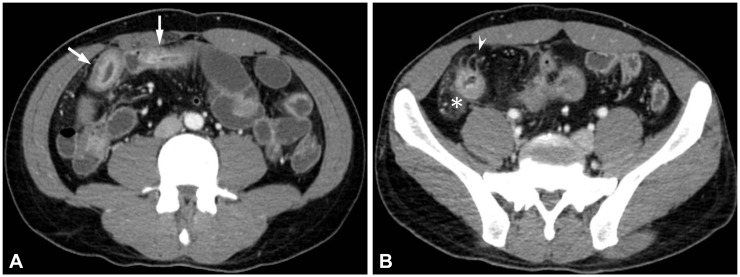
Fig. 1 Active inflammatory Crohn disease in a 28-year-old man. (A) Axial computed tomography enterography images demonstrate multifocal segmental mural hyperenhancement and trilaminar mural stratification in the ileum (arrows), suggesting active disease. (B) Also note engorged vasa recta (arrowheads) and increased attenuation of the mesenteric fat (asterisk).
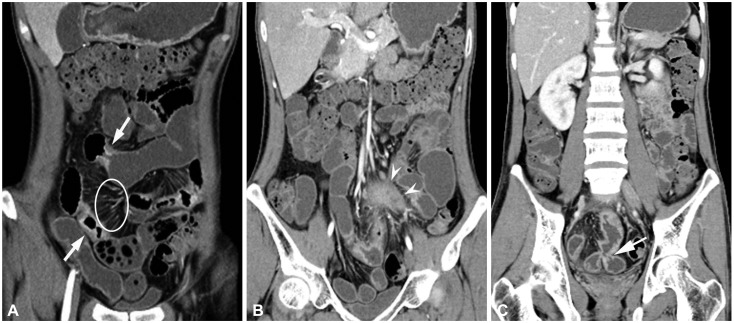
Fig. 2 Active inflammatory Crohn disease with extraenteric complications in a 29-year-old man. (A) Coronal computed tomography enterography images demonstrate multifocal segmental stricture showing wall thickening, mural hyperenhancement and stratification (arrows), and engorged vasa recta, "comb sign" (circle). (B, C) Also noted a mesenteric abscess (arrowheads in B) adjacent to the enteroenteric fistula (arrow in C).
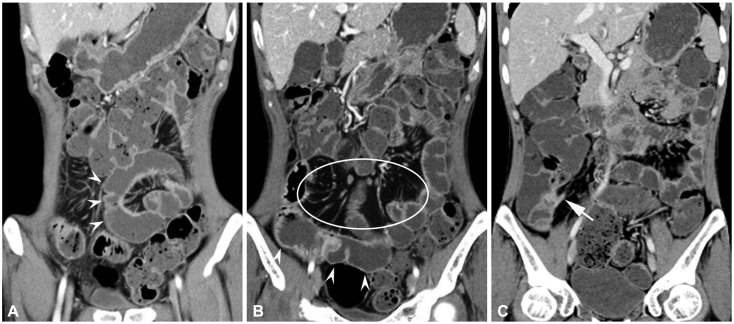
Fig. 3 Crohn disease in a 31-year-old man. (A, B) Coronal computed tomography enterography images show pseudosacculation along the antimesenteric border of small bowel (arrowheads). (B) Fibrofatty proliferation is also demonstrated in the mesentery (circle). (C) Sinus tract arising in the terminal ileum (arrow) which shows mural hyperenhancement and stratification, suggesting active inflammatory disease, is also noted.
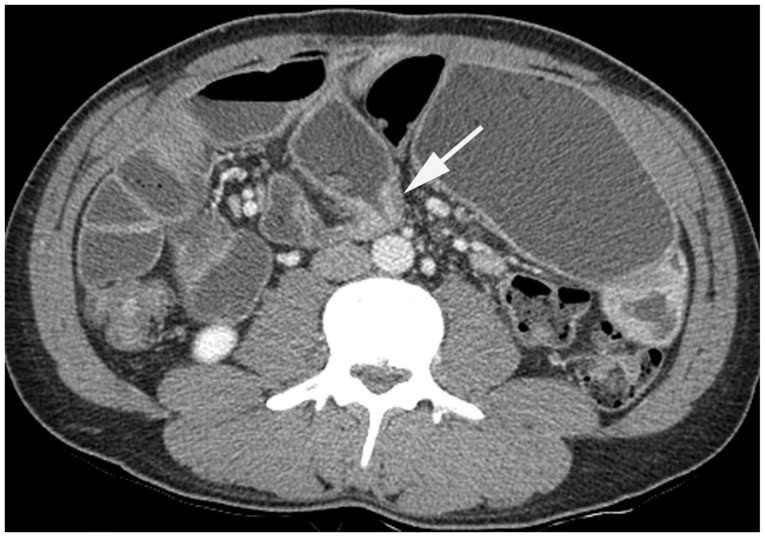
Fig. 4 Fibrostenosing Crohn disease in a 32-year-old man. Axial computed tomography enterography image shows a segmental stricture involving proximal ileal loop. Homogenous mural thickening is seen at the strictured segment without mural hyperenhancement, suggesting fibrostenotic disease (arrow).
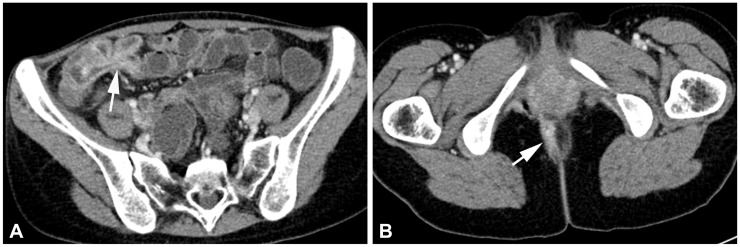
Fig. 5 Crohn disease in a 34-year-old woman. (A) Axial computed tomography enterography image shows enteroenteric fistula involving ileal loops (arrow). (B) Perianal fistula is also seen (arrow).

Fig. 6 Intestinal tuberculosis in a 37-year-old woman. Coronal computed tomography enterography image shows circumferential wall thickening in the ileocecal valve area (arrow). Such ileocecal involvement is the most common form of intestinal tuberculosis.

Fig. 7 Intestinal tuberculosis in a 52-year-old woman. Coronal computed tomography enterography image shows two short segmental circumferential enhancing wall thickenings involving proximal ileal loop (arrows). Associated prestenotic bowel dilatation is also seen.
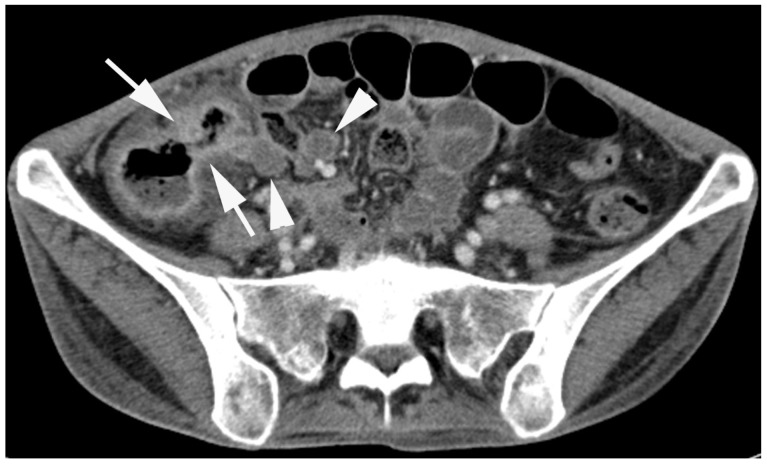
Fig. 8 Intestinal tuberculosis in a 27-year-old woman. Axial computed tomography enterography image shows enhanced wall thickening involving cecum and terminal ileum with patulous ileocecal valve (arrows). Associated central low attenuated lymph nodes are seen at the ileocecal mesentery, suggesting caseous necrosis (arrowheads).

Fig. 9 Crohn disease mimicking intestinal tuberculosis in a 53-year-old man. Relatively short segmental circumferential stricture is suspected in the distal ileal loop (arrow). Associated angulation is also seen. There is no remarkable finding in the mesentery. Preoperative computed tomography diagnosis was intestinal tuberculosis, but Crohn disease was confirmed after segmental resection of the small bowel loop.

Fig. 10 Behcet disease in a 53-year-old woman. Axial computed tomography enterography image shows focal wall thickening with a deep penetrating ulcer (arrowheads) in the terminal ileum, and mesenteric fat infiltration around the ileocecal area.
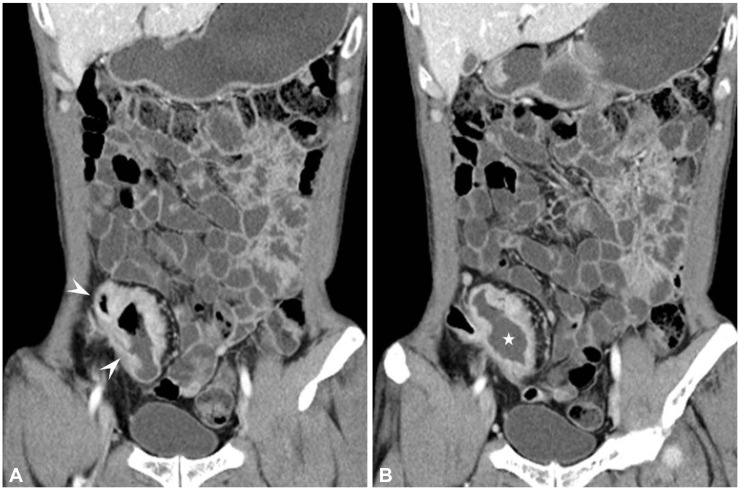
Fig. 11 Behcet disease in a 41-year-old man. (A, B) Axial computed tomography enterography images show wall thickening and several large, deep ulcers (arrowheads in A) in the terminal ileum with aneurysmal dilatation (asterisk in B).

Fig. 12 Recurrent Behcet disease in a 30-year-old woman. Coronal computed tomography enterography image shows an ulceration with peripheral enhancement at the anastomosis site of ileocecectomy (arrows).
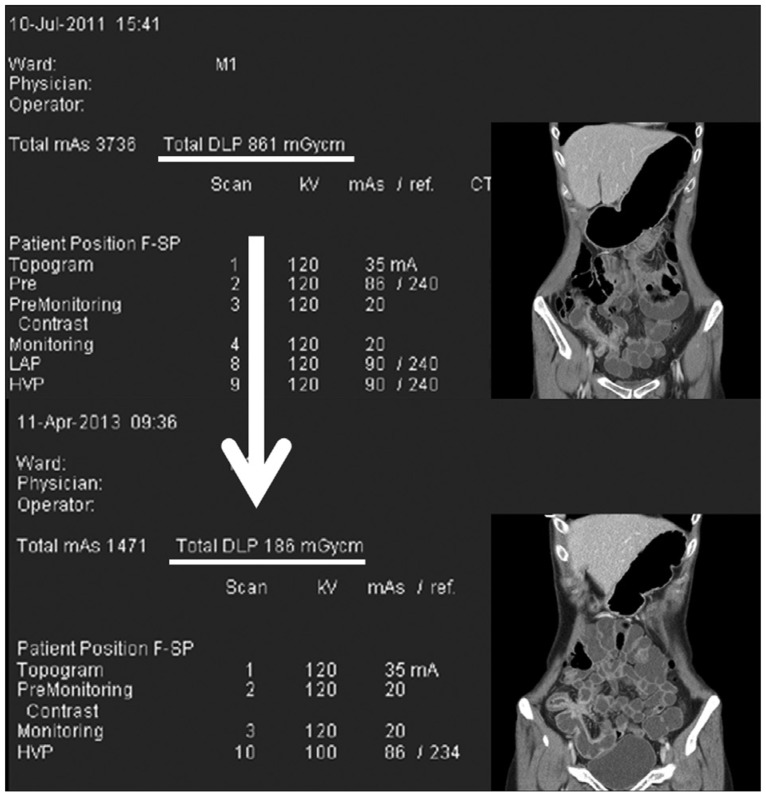
Fig. 13 Radiation dose reduction by application of advanced techniques and computed tomography (CT) protocol optimization. Total dose-length product (DLP) was 861 mGycm in CT enterography (CTE) obtained in 2011 (upper row). Follow-up CTE was taken in the same patient with Crohn disease in 2013. Total DLP was remarkably decreased as 186 mGycm (lower row). In the recent CTE exam, tube current modulation, lowering tube potential, and iterative reconstruction techniques were applied. Only singe portal phase imaging was performed, whereas dual dynamic phases had been obtained in 2011. The similar image quality can be identified, comparing picture-in-picture images.
Reference
-
1. Raptopoulos V, Schwartz RK, McNicholas MM, Movson J, Pearlman J, Joffe N. Multiplanar helical CT enterography in patients with Crohn's disease. AJR Am J Roentgenol. 1997; 169:1545–1550. PMID: 9393162.
Article2. Minordi LM, Vecchioli A, Mirk P, Bonomo L. CT enterography with polyethylene glycol solution vs CT enteroclysis in small bowel disease. Br J Radiol. 2011; 84:112–119. PMID: 20959377.3. Maglinte DD, Sandrasegaran K, Lappas JC, Chiorean M. CT enteroclysis. Radiology. 2007; 245:661–671. PMID: 18024448.
Article4. Stange EF, Travis SP, Vermeire S, et al. European evidence based consensus on the diagnosis and management of Crohn's disease: definitions and diagnosis. Gut. 2006; 55(Suppl 1):i1–i15. PMID: 16481628.
Article5. Meyers MA, McGuire PV. Spiral CT demonstration of hypervascularity in Crohn disease: "vascular jejunization of the ileum" or the "comb sign". Abdom Imaging. 1995; 20:327–332. PMID: 7549737.
Article6. Paulsen SR, Huprich JE, Fletcher JG, et al. CT enterography as a diagnostic tool in evaluating small bowel disorders: review of clinical experience with over 700 cases. Radiographics. 2006; 26:641–657. PMID: 16702444.
Article7. Booya F, Fletcher JG, Huprich JE, et al. Active Crohn disease: CT findings and interobserver agreement for enteric phase CT enterography. Radiology. 2006; 241:787–795. PMID: 17032911.
Article8. Hara AK, Alam S, Heigh RI, Gurudu SR, Hentz JG, Leighton JA. Using CT enterography to monitor Crohn's disease activity: a preliminary study. AJR Am J Roentgenol. 2008; 190:1512–1516. PMID: 18492900.
Article9. Bodily KD, Fletcher JG, Solem CA, et al. Crohn Disease: mural attenuation and thickness at contrast-enhanced CT Enterography: correlation with endoscopic and histologic findings of inflammation. Radiology. 2006; 238:505–516. PMID: 16436815.11. Lee SS, Ha HK, Yang SK, et al. CT of prominent pericolic or perienteric vasculature in patients with Crohn's disease: correlation with clinical disease activity and findings on barium studies. AJR Am J Roentgenol. 2002; 179:1029–1036. PMID: 12239060.
Article12. Colombel JF, Solem CA, Sandborn WJ, et al. Quantitative measurement and visual assessment of ileal Crohn's disease activity by computed tomography enterography: correlation with endoscopic severity and C reactive protein. Gut. 2006; 55:1561–1567. PMID: 16648154.
Article13. Solem CA, Loftus EV Jr, Fletcher JG, et al. Small-bowel imaging in Crohn's disease: a prospective, blinded, 4-way comparison trial. Gastrointest Endosc. 2008; 68:255–266. PMID: 18513722.14. Wills JS, Lobis IF, Denstman FJ. Crohn disease: state of the art. Radiology. 1997; 202:597–610. PMID: 9051003.
Article15. Vogel J, da Luz Moreira A, Baker M, et al. CT enterography for Crohn's disease: accurate preoperative diagnostic imaging. Dis Colon Rectum. 2007; 50:1761–1769. PMID: 17701255.
Article16. Paulsen SR, Huprich JE, Hara AK. CT enterography: noninvasive evaluation of Crohn's disease and obscure gastrointestinal bleed. Radiol Clin North Am. 2007; 45:303–315. PMID: 17502219.
Article17. Desreumaux P, Ernst O, Geboes K, et al. Inflammatory alterations in mesenteric adipose tissue in Crohn's disease. Gastroenterology. 1999; 117:73–81. PMID: 10381912.
Article18. Maglinte DD, Gourtsoyiannis N, Rex D, Howard TJ, Kelvin FM. Classification of small bowel Crohn's subtypes based on multimodality imaging. Radiol Clin North Am. 2003; 41:285–303. PMID: 12659339.
Article19. Schwartz DA, Loftus EV Jr, Tremaine WJ, et al. The natural history of fistulizing Crohn's disease in Olmsted County, Minnesota. Gastroenterology. 2002; 122:875–880. PMID: 11910338.
Article20. Bruining DH, Siddiki HA, Fletcher JG, Tremaine WJ, Sandborn WJ, Loftus EV Jr. Prevalence of penetrating disease and extraintestinal manifestations of Crohn's disease detected with CT enterography. Inflamm Bowel Dis. 2008; 14:1701–1706. PMID: 18623171.
Article21. Bruining DH, Siddiki HA, Fletcher JG, et al. Benefit of computed tomography enterography in Crohn's disease: effects on patient management and physician level of confidence. Inflamm Bowel Dis. 2012; 18:219–225. PMID: 21337477.
Article22. Booya F, Akram S, Fletcher JG, et al. CT enterography and fistulizing Crohn's disease: clinical benefit and radiographic findings. Abdom Imaging. 2009; 34:467–475. PMID: 18551336.
Article23. Wu YW, Tang YH, Hao NX, Tang CY, Miao F. Crohn's disease: CT enterography manifestations before and after treatment. Eur J Radiol. 2012; 81:52–59. PMID: 21185142.
Article24. Wu YW, Tao XF, Tang YH, Hao NX, Miao F. Quantitative measures of comb sign in Crohn's disease: correlation with disease activity and laboratory indications. Abdom Imaging. 2012; 37:350–358. PMID: 22002159.
Article25. Epstein D, Watermeyer G, Kirsch R. Review article: the diagnosis and management of Crohn's disease in populations with high-risk rates for tuberculosis. Aliment Pharmacol Ther. 2007; 25:1373–1388. PMID: 17539977.
Article26. Akhan O, Pringot J. Imaging of abdominal tuberculosis. Eur Radiol. 2002; 12:312–323. PMID: 11870428.
Article27. Makanjuola D. Is it Crohn's disease or intestinal tuberculosis? CT analysis. Eur J Radiol. 1998; 28:55–61. PMID: 9717624.
Article28. Lakhanpal S, Tani K, Lie JT, Katoh K, Ishigatsubo Y, Ohokubo T. Pathologic features of Behcet's syndrome: a review of Japanese autopsy registry data. Hum Pathol. 1985; 16:790–795. PMID: 4018777.29. Sakane T, Takeno M, Suzuki N, Inaba G. Behcet's disease. N Engl J Med. 1999; 341:1284–1291. PMID: 10528040.30. Cheon JH, Kim ES, Shin SJ, et al. Development and validation of novel diagnostic criteria for intestinal Behcet's disease in Korean patients with ileocolonic ulcers. Am J Gastroenterol. 2009; 104:2492–2499. PMID: 19532129.31. Ha HK, Lee HJ, Yang SK, et al. Intestinal Behcet syndrome: CT features of patients with and patients without complications. Radiology. 1998; 209:449–454. PMID: 9807572.32. Chae EJ, Do KH, Seo JB, et al. Radiologic and clinical findings of Behcet disease: comprehensive review of multisystemic involvement. Radiographics. 2008; 28:e31. PMID: 18603663.33. Iida M, Kobayashi H, Matsumoto T, et al. Postoperative recurrence in patients with intestinal Behcet's disease. Dis Colon Rectum. 1994; 37:16–21. PMID: 8287741.34. Kasahara Y, Tanaka S, Nishino M, Umemura H, Shiraha S, Kuyama T. Intestinal involvement in Behcet's disease: review of 136 surgical cases in the Japanese literature. Dis Colon Rectum. 1981; 24:103–106. PMID: 7215071.35. Ghonge NP, Aggarwal B, Gothi R. CT enterography: state-of-the-art CT technique for small bowel imaging. Indian J Gastroenterol. 2013; 32:152–162. PMID: 23475544.
Article36. Desmond AN, O'Regan K, Curran C, et al. Crohn's disease: factors associated with exposure to high levels of diagnostic radiation. Gut. 2008; 57:1524–1529. PMID: 18443021.
Article37. Jung YS, Park DI, Kim ER, et al. Quantifying exposure to diagnostic radiation and factors associated with exposure to high levels of radiation in Korean patients with inflammatory bowel disease. Inflamm Bowel Dis. Epub 2013 May 22. DOI: 10.1097/MIB.0b013e31828c844f.
Article38. Lee CH, Goo JM, Ye HJ, et al. Radiation dose modulation techniques in the multidetector CT era: from basics to practice. Radiographics. 2008; 28:1451–1459. PMID: 18794318.
Article39. Yu L, Bruesewitz MR, Thomas KB, Fletcher JG, Kofler JM, McCollough CH. Optimal tube potential for radiation dose reduction in pediatric CT: principles, clinical implementations, and pitfalls. Radiographics. 2011; 31:835–848. PMID: 21571660.
Article40. Kaza RK, Platt JF, Al-Hawary MM, Wasnik A, Liu PS, Pandya A. CT enterography at 80 kVp with adaptive statistical iterative reconstruction versus at 120 kVp with standard reconstruction: image quality, diagnostic adequacy, and dose reduction. AJR Am J Roentgenol. 2012; 198:1084–1092. PMID: 22528897.
Article41. Wold PB, Fletcher JG, Johnson CD, Sandborn WJ. Assessment of small bowel Crohn disease: noninvasive peroral CT enterography compared with other imaging methods and endoscopy: feasibility study. Radiology. 2003; 229:275–281. PMID: 12944602.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Computed Tomography Enterography and Magnetic Resonance Enterography in the Diagnosis of Crohn's Disease
- Role of Computed Tomography Enterography/Magnetic Resonance Enterography: Is It in Prime Time?
- A Look into the Small Bowel in Crohn's Disease
- Preparation, Technique, and Imaging of Computed Tomography/Magnetic Resonance Enterography
- The role of small bowel endoscopy in small bowel Crohn's disease: when and how?
