Four-Dimensional CT of the Diaphragm in Children: Initial Experience
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul 05505, Korea. ghw68@hanmail.net
- KMID: 2425116
- DOI: http://doi.org/10.3348/kjr.2018.19.1.111
Abstract
OBJECTIVE
To evaluate the technical feasibility of four-dimensional (4D) CT for the functional evaluation of the pediatric diaphragm.
MATERIALS AND METHODS
In 22 consecutive children (median age 3.5 months, age range 3 days-3 years), 4D CT was performed to assess diaphragm motion. Diaphragm abnormalities were qualitatively evaluated and diaphragm motion was quantitatively measured on 4D CT. Lung density changes between peak inspiration and expiration were measured in the basal lung parenchyma. The diaphragm motions and lung density changes measured on 4D CT were compared between various diaphragm conditions. In 11 of the 22 children, chest sonography was available for comparison.
RESULTS
Four-dimensional CT demonstrated normal diaphragm (n = 8), paralysis (n = 10), eventration (n = 3), and diffusely decreased motion (n = 1). Chest sonography demonstrated normal diaphragm (n = 2), paralysis (n = 6), eventration (n = 2), and right pleural effusion (n = 1). The sonographic findings were concordant with the 4D CT findings in 90.9% (10/11) of the patients. In diaphragm paralysis, the affected diaphragm motion was significantly decreased compared with the contralateral normal diaphragm motion (−1.1 ± 2.2 mm vs. 7.6 ± 3.8 mm, p = 0.005). The normal diaphragms showed significantly greater motion than the paralyzed diaphragms (4.5 ± 2.1 mm vs. −1.1 ± 2.2 mm, p < 0.0001), while the normal diaphragm motion was significantly smaller than the motion of the contralateral normal diaphragm in paralysis (4.5 ± 2.1 mm vs. 7.6 ± 3.8 mm, p = 0.01). Basal lung density change of the affected side was significantly smaller than that of the contralateral side in diaphragm paralysis (89 ± 73 Hounsfield units [HU] vs. 180 ± 71 HU, p = 0.03), while no significant differences were found between the normal diaphragms and the paralyzed diaphragms (136 ± 66 HU vs. 89 ± 73 HU, p = 0.1) or between the normal diaphragms and the contralateral normal diaphragms in paralysis (136 ± 66 HU vs. 180 ± 71 HU, p = 0.1).
CONCLUSION
The functional evaluation of the pediatric diaphragm is feasible with 4D CT in select children.
Keyword
MeSH Terms
Figure
-

Fig. 1 3-day-old female newborn with congenital pulmonary airway malformation.Coronal reformatted 4D CT images using thin-slab averaging technique obtained at peak inspiration (A) and peak expiration (B) demonstrate synchronous motion (arrows) of both diaphragms (right, 1.6 mm; left 1.8 mm). 4D = four-dimensional
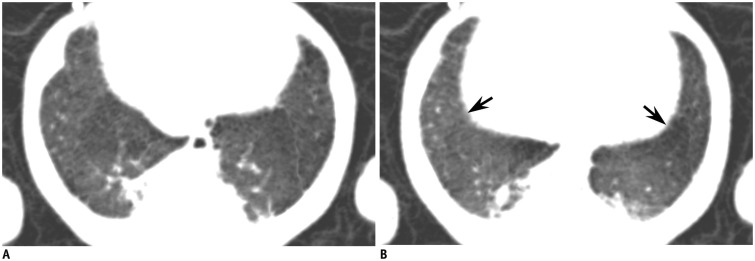
Fig. 2 4-month-old male infant with chronic lung disease.Oblique axial reformatted 4D CT minimum intensity projection images obtained at peak inspiration (A) and peak expiration (B) show simultaneous respiratory excursion (arrows) of both diaphragms (right, 4.8 mm; left 3.3 mm). Lung parenchymal lesions related to chronic lung disease are noted in posteromedial portions of both basal lungs.
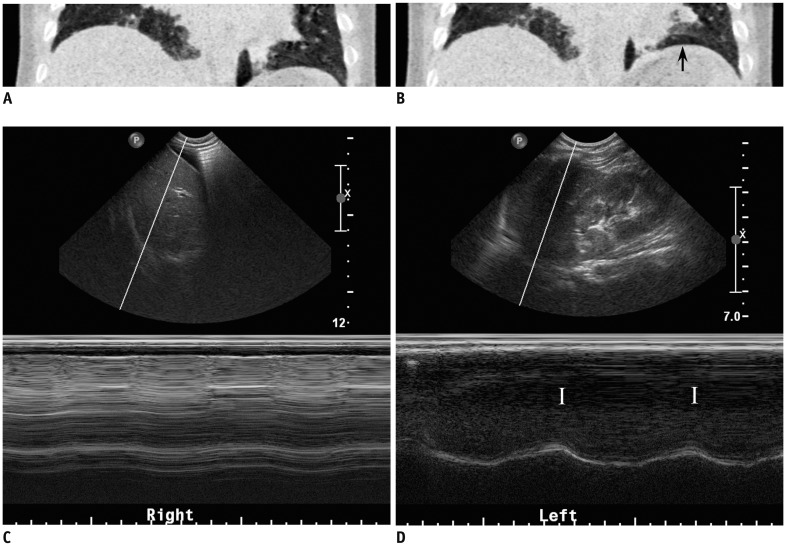
Fig. 3 7-month-old male infant with double-outlet right ventricle, ventricular septal defect, and interrupted aortic arch who underwent aortic arch repair followed by pulsatile, bidirectional, cavopulmonary connection.Coronal reformatted 4D CT minimum intensity projection images obtained at peak inspiration (A) and peak expiration (B) reveal almost no change in position of right diaphragm (1.8 mm) indicating right diaphragm paralysis. Left diaphragm shows normal motion (10.8 mm, arrow). C. M-mode sonography also shows almost no motion of right diaphragm as in 4D CT. D. M-mode sonography displays normal motion of left diaphragm with inspiration peaks (I).
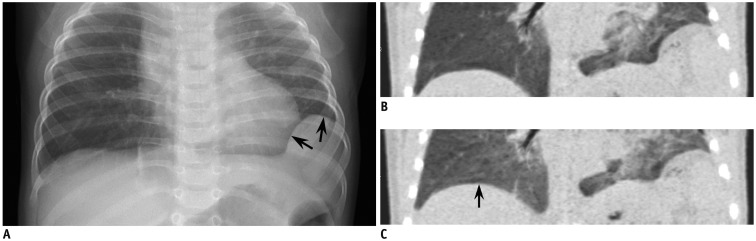
Fig. 4 6-month-old female infant with left diaphragmatic eventration.(A) Anteroposterior chest radiography shows focal bulge (arrows) at lateral portion of left diaphragm suggesting diaphragm eventration. Subsegmental atelectasis is noted in right basal lung. Coronal reformatted 4D CT minimum intensity projection images obtained at peak inspiration (B) and peak expiration (C) demonstrate markedly reduced motion of affected portion of left diaphragm (0.8 mm) as well as preserved motion of medial portion of left diaphragm (4.7 mm). Respiratory excursion (arrow) of normal right diaphragm was measured as 5.1 mm.
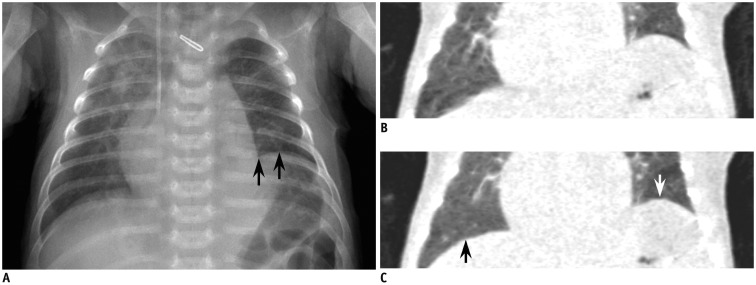
Fig. 5 24-day-old male newborn who underwent aortic arch repair for interrupted aortic arch.(A) Anteroposterior chest radiography reveals elevated left diaphragm (arrows) due to phrenic nerve injury during cardiac surgery. Increased opacities probably due to atelectasis in both lung fields, right central venous catheter, and surgical clip at aortic arch repair site are noted. Coronal reformatted 4D CT minimum intensity projection images obtained at peak inspiration (B) and peak expiration (C) demonstrate normal motion (black arrow) of right diaphragm (4.7 mm) and paradoxical motion (white arrow) of paralyzed left diaphragm (− 5.1 mm).
Cited by 2 articles
-
Four-Dimensional Thoracic CT in Free-Breathing Children
Hyun Woo Goo
Korean J Radiol. 2019;20(1):50-57. doi: 10.3348/kjr.2018.0325.User-Friendly Vendor-Specific Guideline for Pediatric Cardiothoracic Computed Tomography Provided by the Asian Society of Cardiovascular Imaging Congenital Heart Disease Study Group: Part 1. Imaging Techniques
Sun Hwa Hong, Hyun Woo Goo, Eriko Maeda, Ki Seok Choo, I-Chen Tsai,
Korean J Radiol. 2019;20(2):190-204. doi: 10.3348/kjr.2018.0571.
Reference
-
1. Nason LK, Walker CM, McNeeley MF, Burivong W, Fligner CL, Godwin JD. Imaging of the diaphragm: Anatomy and function. Radiographics. 2012; 32:E51–E70. PMID: 22411950.
Article2. Kharma N. Dysfunction of the diaphragm: imaging as a diagnostic tool. Curr Opin Pulm Med. 2013; 19:394–398. PMID: 23715292.3. Chavhan GB, Babyn PS, Cohen RA, Langer JC. Multimodality imaging of the pediatric diaphragm: anatomy and pathologic conditions. Radiographics. 2010; 30:1797–1817. PMID: 21057121.
Article4. Epelman M, Navarro OM, Daneman A, Miller SF. M-mode sonography of diaphragmatic motion: description of technique and experience in 278 pediatric patients. Pediatr Radiol. 2005; 35:661–667. PMID: 15776227.
Article5. Goo HW. Advanced functional thoracic imaging in children: from basic concepts to clinical applications. Pediatr Radiol. 2013; 43:262–268. PMID: 23417252.
Article6. Ayoub J, Cohendy R, Dauzat M, Targhetta R, De la Coussaye JE, Bourgeois JM, et al. Non-invasive quantification of diaphragm kinetics using m-mode sonography. Can J Anaesth. 1997; 44:739–744. PMID: 9232305.
Article7. Greenberg SB. Dynamic pulmonary CT of children. Am J Roentgenol. 2012; 199:435–440. PMID: 22826409.
Article8. Goo HW. Current trends in cardiac CT in children. Acta Radiol. 2013; 54:1055–1062. PMID: 23104372.
Article9. Tan JZ, Crossett M, Ditchfield M. Dynamic volumetric computed tomographic assessment of the young paediatric airway: Initial experience of rapid, non-invasive, four-dimensional technique. J Med Imaging Radiat Oncol. 2013; 57:141–148. PMID: 23551770.
Article10. Greenberg SB, Dyamenahalli U. Dynamic pulmonary computed tomography angiography: a new standard for evaluation of combined airway and vascular abnormalities in infants. Int J Cardiovasc Imaging. 2014; 30:407–414. PMID: 24322888.
Article11. Goo HW. Individualized volume CT dose index determined by cross-sectional area and mean density of the body to achieve uniform image noise of contrast-enhanced pediatric chest CT obtained at variable kV levels and with combined tube current modulation. Pediatr Radiol. 2011; 41:839–847. PMID: 21656275.
Article12. Goo HW, Kim HJ. Detection of air trapping on inspiratory and expiratory phase images obtained by 0.3-second cine CT in the lungs of free-breathing young children. Am J Roentgenol. 2006; 187:1019–1023. PMID: 16985151.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Usefulness of Two-dimensioanl CT & Three-dimensional CT in Blow-out Fracture
- Traumatic Rupture of the Diaphragm: CT Findings
- Anterior Diaphragm Below the Xiphoid Process: CT Finding
- Abnormalities of Diaphragm and Adjacent Structures: Usefulness of Ultrasonography
- Four-Dimensional Thoracic CT in Free-Breathing Children
