Mycotic Cerebral Aneurysms Secondary to Scedosporium Prolificans Infection in a Patient with Multiple Sclerosis
- Affiliations
-
- 1Department of Neurology, University General Hospital, Ciudad Real, Spain. mavagua_24@hotmail.com
- 2Department of Anatomical Pathology, University General Hospital, Ciudad Real, Spain.
- KMID: 2424198
- DOI: http://doi.org/10.3988/jcn.2018.14.4.601
Abstract
- No abstract available.
Figure
-
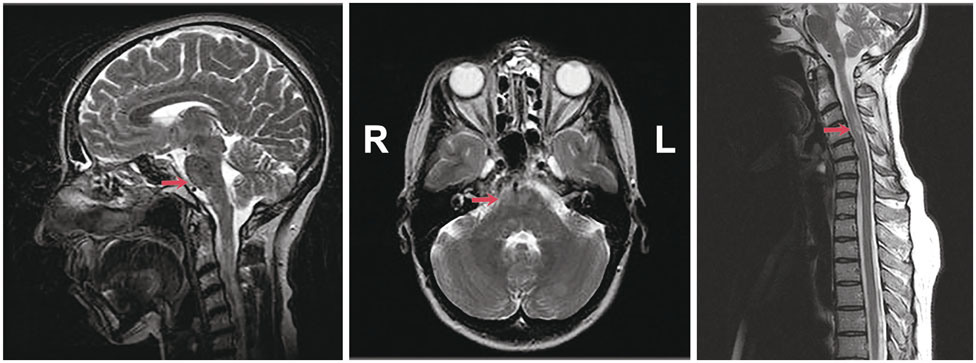
Fig. 1 MRI T2-weighted images showing hyperintensities (arrows) in the brainstem and spinal cord. A: Brainstem, sagittal view. B: Brainstem, axial view. C: Spinal cord, sagittal view.
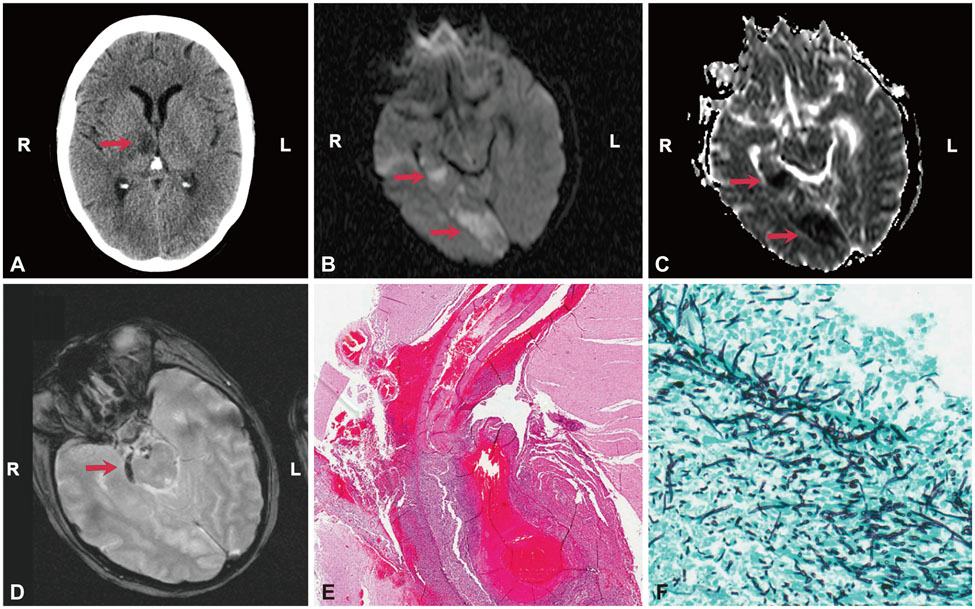
Fig. 2 Composition of CT scan (A), MRI (B–D), and anatomical pathology (E–F) images. A: CT image obtained at admission showing thalamic hypodensity (arrow). B: Hyperintensities in MRI long-repetition-time images with (C) restricted diffusion in medial temporal and occipital lobes (arrows). D: MRI gradient-echo images displaying small subarachnoid hemorrhage foci in the interpeduncular cistern and anterior to the right cerebral peduncle (arrow). E: Microscopy image revealing necrosis and rupture of the arterial wall of the basilar artery, in which a ruptured aneurysm dilatation and a vascular thrombus are evident (hematoxylin-eosin stain, ×20). F: Methenamine silver staining showing multiple fungal structures identified as Scedosporium prolificans in the necrotic areas (×400).
Reference
-
1. Malloch D, Salkin IF. A new species of Scedosporium associated with osteomyelitis in humans. Mycotaxon. 1984; 21:247–255.2. Marco de Lucas E, Sádaba P, Lastra García-Barón P, Ruiz Delgado ML, Cuevas J, Salesa R, et al. Cerebral scedosporiosis: an emerging fungal infection in severe neutropenic patients: CT features and CT pathologic correlation. Eur Radiol. 2006; 16:496–502.
Article3. Rodriguez-Tudela JL, Berenguer J, Guarro J, Kantarcioglu AS, Horre R, de Hoog GS, et al. Epidemiology and outcome of Scedosporium prolificans infection, a review of 162 cases. Med Mycol. 2009; 47:359–370.
Article4. Idigoras P, Pérez-Trallero E, Piñeiro L, Larruskain J, López-Lopategui MC, Rodríguez N, et al. Disseminated infection and colonization by Scedosporium prolificans: a review of 18 cases, 1990-1999. Clin Infect Dis. 2001; 32:E158–E165.
Article5. Ong A, Blyth CC, Bency R, Vicaretti M, Harun A, Meyer W, et al. Fatal mycotic aneurysms due to Scedosporium and Pseudoallescheria infection. J Clin Microbiol. 2011; 49:2067–2071.
Article6. Díaz-Valle D, Benitez del Castillo JM, Amor E, Toledano N, Carretero MM, Díaz-Valle T. Severe keratomycosis secondary to Scedosporium apiospermum. Cornea. 2002; 21:516–518.
Article7. National Medical Advisory Board of the National Multiple Sclerosis Society. Recommendations regarding corticosteroids in the management of multiple sclerosis. US Neurology. 2008; 4:22–24.8. Franchin G, Diamond B. Pulse steroids: how much is enough? Autoimmun Rev. 2006; 5:111–113.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Scedosporium prolificansInfection by Laceration with a Broken Piece of Flowerpot: A Case Report
- A Case of Fatal Scedosporium prolificans Fungemia in a Patient with Acute Myeloid Leukemia
- A Middle Cerebral Mycotic Aneurysm Ruptured into the Lateral Ventricle
- A Case of Infective Endocarditis with Mycotic Aneurysms
- Peripheral Cerebral Arterial Aneurysm: Case Report and Review of the Literature
