Change of Femoral Anteversion during Closed Femoral Intramedullary Nailing
- KMID: 2423598
- DOI: http://doi.org/10.4055/jkoa.1996.31.2.218
Abstract
- Average anteversion of the femur is 15.3 degree. Ultrasound, computerized tomogram, and three dimensional reconstruction from CT or MRI have been used for more accurate measurement of the anteversion. There are two methods in measuing anteversion angle from CT scan:one is by drawing a mid line through long axis of the femoral neck (conventional method). Another is by drawing a line from the center of the head to that of the neck at the base of the trochanter using several cut slices (Murphy's method). We compared these methods with fluoroscopic measurement of the Anteversion. We traced the change of the anteversion before and after closed femoral intramedullary (IMO) nailing to evaluate the origin of malrotation of the femur. 1. Normal anteversion angles were measured in 15 cases. Average anteversion angle was 6.9 degrees by conventional method, 12.3 degrees by Murphy's method, and 12.2 degrees by fluoroscope. 2. Anteversion angles were measured after IM nailing in 18 cases. Average was 17 degrees by Murphy's method and 15.2 degrees by fluoroscope. Mean of difference between these two methods sea 6.3 degrees. That was 1.7 degrees in normal side. 3. Change of the anteversion angle between before and after IM nailing was measured in 17 cases by fluoroscope. Average anteversion angle before the operation was 11.9 degrees and it was change to 15.8 degrees after operation. Mean of these change was 7.1 degrees. 4. Pereperative traction provides important information on change of anteversion. Reduction excessive flexion of proximal fragment was a origin of change of anteversion during nailing procedure. Conclusion : Malrotation of the femur after IM nailing must be keep in mind and it may be preventable by fluoroscopic control of the rotation in nailing procedure.
Keyword
MeSH Terms
Figure
-
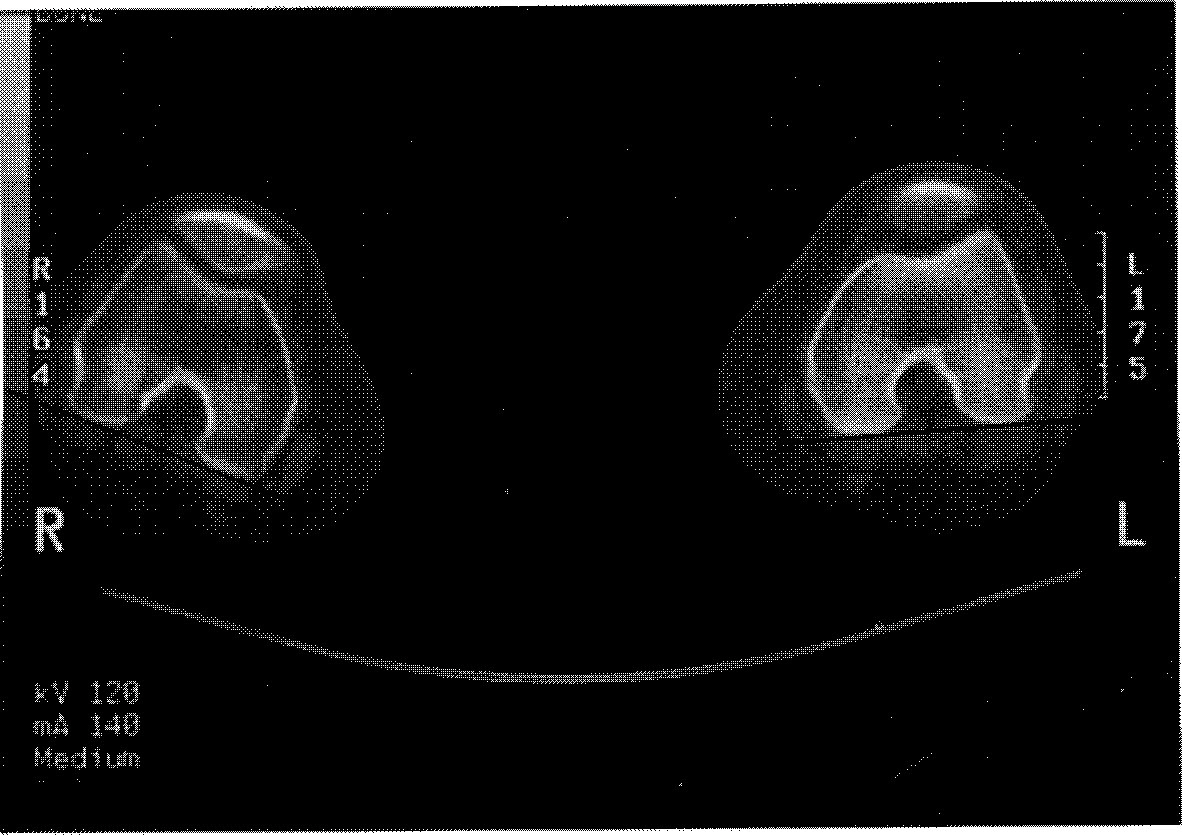
Fig. 1 Computerized tomography of distal end of the femur. The reference line passes through posterior margins of both condyles.
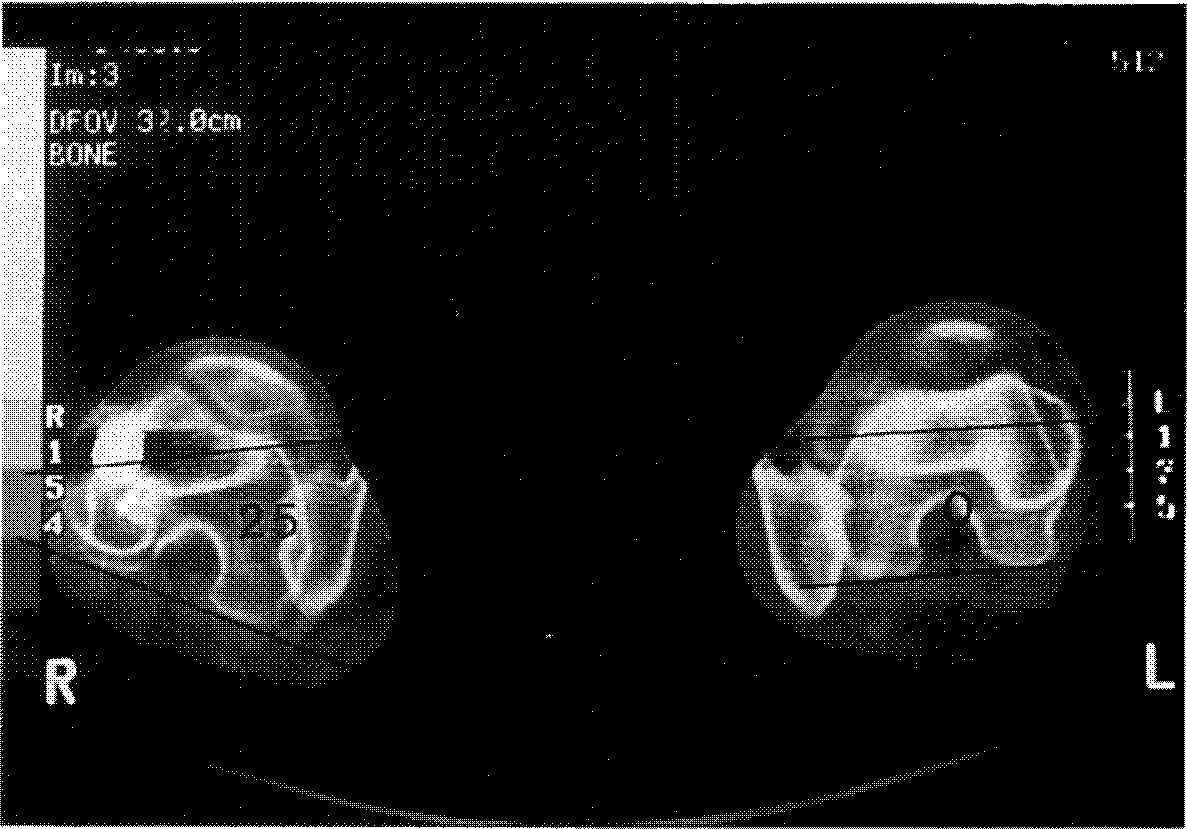
Fig. 2 Computerized tomographies of the femoral neck and condyles are overlapped, Angle between the reference line (posterior margin of both condyles) and the femoral neck line is regarded as an anteversion of the femur.

Fig. 3 Computerized tomographies of the femoral head and neck are over lapped. Angle between the reference line (posterior margin of both condyles) and the line connecting center of the head and neck is regarded as an anteversion (Murphy’ method) of the femur.
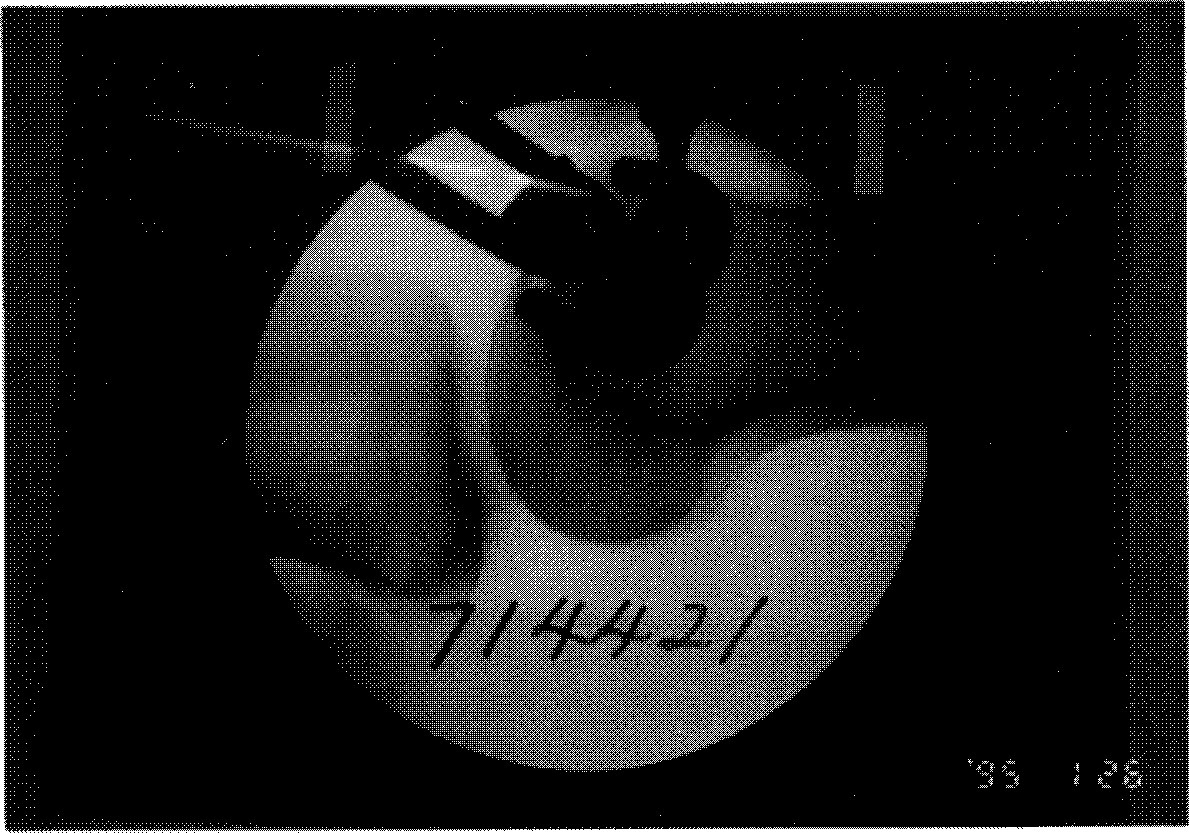
Fig. 4 Visualization of distal femoral condyle by image intensifier. Posterior margin of both femoral condyles was overlapped to confirm the neutral position of the distal fragment.
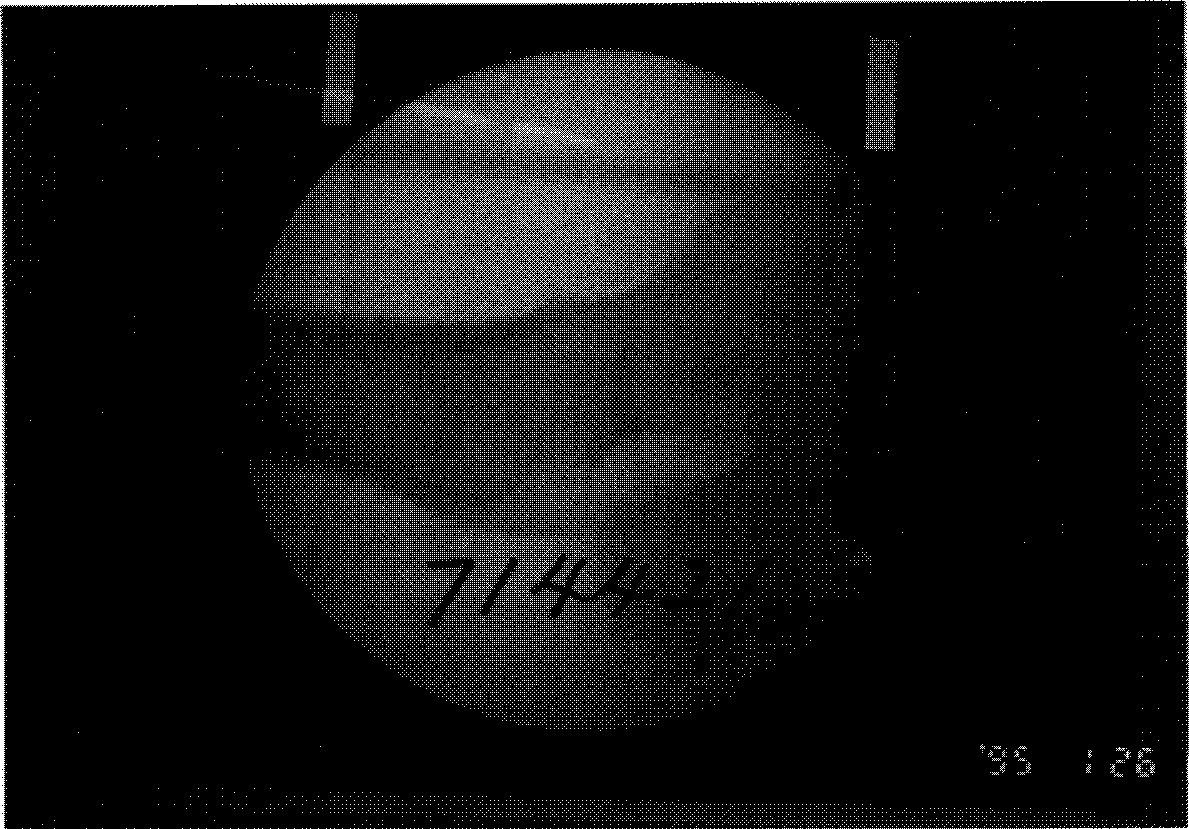
Fig. 5 Preoperative visualization of the proximal femur by image intensifier. Angle of the neck was an anteversion of the femur.
Fig. 6 Postoperative visualization of the proximal femur by image intensifier. Angle of the neck was an anteversion of the femur.
Reference
-
3. Braten M,, Terjesen T, Rossvoll I. Femoral anteversion in normal adults: Ultrasound measurements in 50 men and 50 women. Acta Orthop Scand. 1992; 63:29–32.4. Braten M, Terjesen T, Rossvoll I. Torsional deformity after intramedullary nailing of femoral shaft fractures. J Borne Joint Surg. 1993; 75-B:799–803.5. Klemm K, Schnellmann WD. Dynamische and Statische Verriegelung des Marknagels Monatssehr. Unfallheik. 1972; 75:568–575.6. Murphy SB, Simon SR, Kijewski PK, Wilkinson RH, Griscom NT. Femoral anteversion. J Bone Joint Surg. 69-A:1169–1176. 1987.
Article7. Reikeras O, Bjerkreim I, Kolbenstvedt A. Anteversion of the acetabulum and femoral neck in normals and in patients with osteoarthritis of the hip. Acta Orthop Scand. 1983; 54:18–23.8. Sennerich T, Sutter P., Ritter G, Zapf S. Computertomographisch Kontrolle des Antetorsionwinkels nach Oberschenkelschaftfrankturen des Erwachsenen. Unfallchiurg. 1992; 95:301–305.9. Tachdjian MO. Pediatric Orthopedics. The foot and leg. 1990. Second ed. W.B.: Saunders Co.;p. 2800–2810.10. Winquist RA, Hansen ST, Clawson DK. Closed Intramedullary Nailing of Femoral Fractures. J Bone Joint Surg. 1984; 66-A:529–539.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Fracture of Femur Neck Associated with Technical Errors in Closed Intramedullary Nailing of the Femur
- Malrotation Deformity Following Intramedullary Nailing in Femoral Shaft Fracture - Does True Neutral Rotation of the Distal Fragment Prevent the Deformity?
- Rotational Deformity after Closed Interlocking nailing of Femoral Fracture
- Closed Intramedullary Nailing of Femoral Shaft Fractures
- Treatment of the Fractures of the Shaft of the Femur with Intramedullary Nailing
