Pelvic Osteotomy in Adults
- Affiliations
-
- 1Department of Orthopaedic Surgery, College of Medicine, Kyung Hee University, Seoul, Korea. yjcho@khmc.or.kr
- KMID: 2421343
- DOI: http://doi.org/10.4055/jkoa.2017.52.6.500
Abstract
- Pelvic osteotomy is a surgery for correcting acetabular deformity, which causes incomplete coverage of the femoral head or biomechanically abnormal load to the hip joint. Pelvic osteotomy can be divided into two categories: reconstructive or realignment osteotomy and salvage osteotomy. Reconstructive osteotomy can be performed to correct the dysplastic hip with good congruency, and include most pelvic osteotomies, except Chiari osteotomy. Among these, Bernese osteotomy, rotational acetabular osteotomy, and periacetabular rotational osteotomy are commonly being used. Salvage osteotomy, which include Chiari osteotomy only, can be performed to increase the coverage of the femoral head of hip joint with joint incongruency due to the severely deformed femoral head and acetabulum or advanced osteoarthritis. Chiari osteotomy is a kind of arthroplasty reducing the pressure applied to the head, and increasing the bone coverage on the upper part of the femoral head. It is effective in reducing hip pain and slowing degenerative changes; however, as the surface is covered by fibrous cartilage, it is vulnerable to degenerative changes. The pelvic osteotomy is a very important and useful surgical technique to preserve joints, despite being a difficult procedure that is technically demanding.
Keyword
MeSH Terms
Figure
-
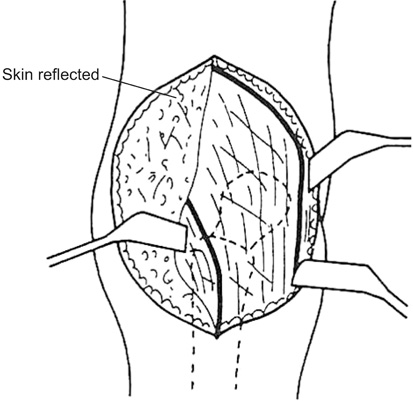
Figure 1 Skin incision and approach of rotational acetabular osteotomy. Cited from Ninomiya and Tagawa (J Bone Joint Surg Am. 1984;66:430-6).9)
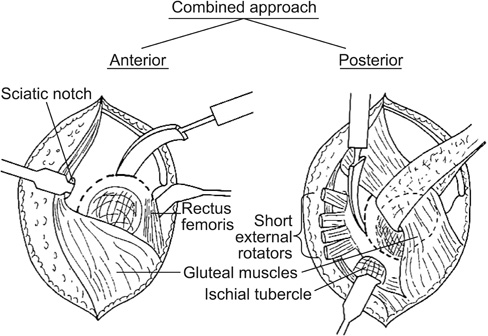
Figure 2 Approach of rotational acetabular osteotomy. This approach combines the anterior iliofemoral and posterior approaches through a single skin incision. Cited from Ninomiya and Tagawa (J Bone Joint Surg Am. 1984;66:430-6).9)
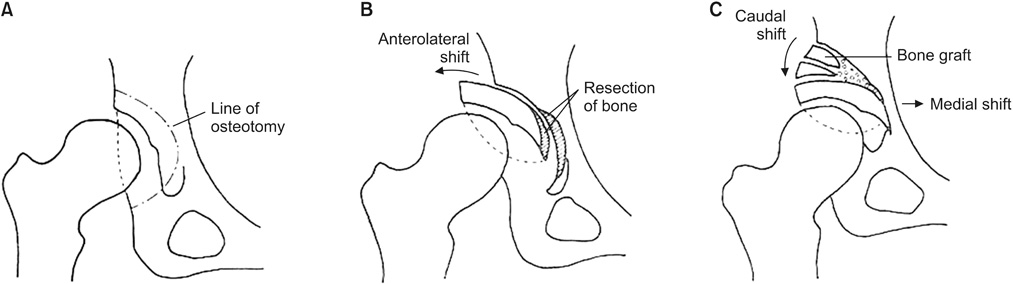
Figure 3 Schematic drawing of the operative procedure. The freed acetabulum should be shifted anterolaterally, medially, and downward. (A) Preoperative view. (B) Anterolateral shift. (C) Downward and medial shift after removal of the excess bone. Cited from Ninomiya and Tagawa (J Bone Joint Surg Am. 1984;66:430-6).9)
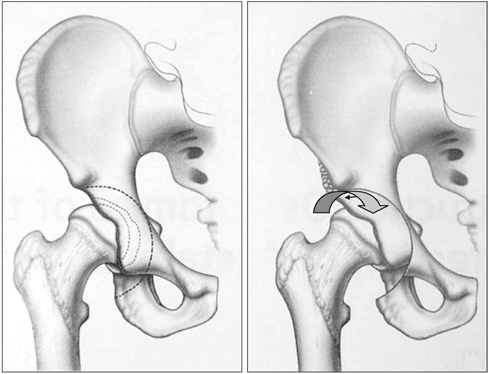
Figure 4 Transpositional osteotomy. Rotation of the acetabulum is focused on anterior rotation.
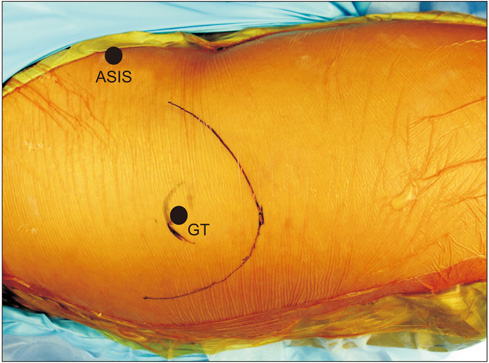
Figure 5 Drawing of skin incision line of modified Ollier transtrochanteric approach. ASIS, anterior superior iliac spine; GT, greater trochanter

Figure 6 Osteotomy greater trochanter using a Gigli saw. (A) Draw an osteotomy line and perform osteotomy along the line using Gigli saw. (B) After osteotomy, the fragment of the greater trochanter and abductor muscle is retracted proximally.
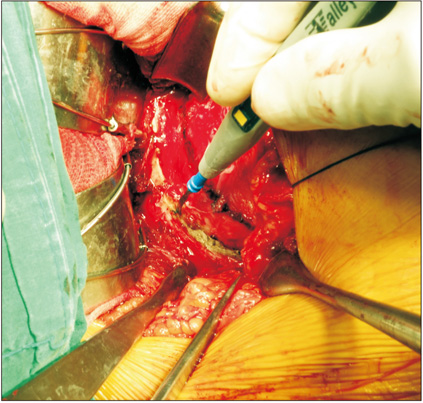
Figure 7 Draw a completely circular osteotomy line 1 cm away from acetabular rim.

Figure 8 (A) Perform osteotomy of the ilium along the osteotomy line, first using a round osteotome. (B) Perform osteotomy ischium along the osteotomy line.

Figure 9 Osteotomy of the pubis is performed blindly by an approach between the hip joint capsule and rectus femoris. (A) Release rectus femoris muscle from the hip joint capsule using a periosteum elevator. (B) Osteotomy site of the pubis is pectineal eminence of the pubis. Iliopsoas tendon should be retracted medially by a small Hohman retractor during osteotomy of the pubis.
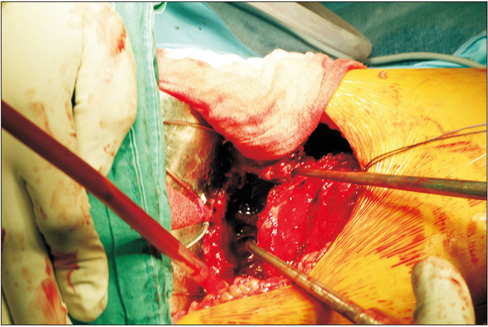
Figure 10 Rotate acetbular fragment anteriorly and laterally using bone hook.
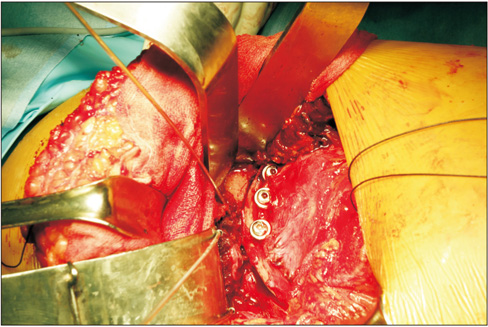
Figure 11 Fix the acetabular fragment using 2, 3, or 3.5 mm cortical screws.
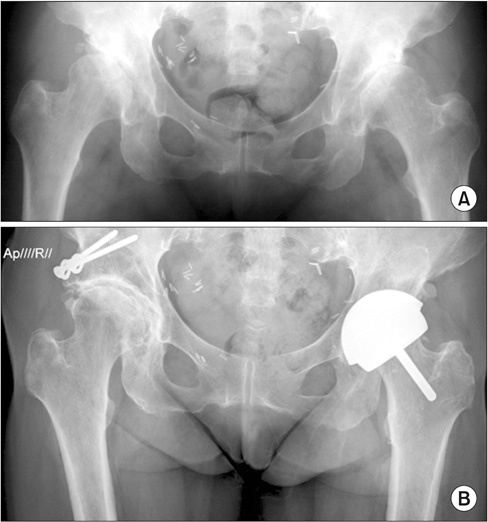
Figure 12 (A) Preoperative both hip anteroposterior radiograph of a 45-year-old woman showing bilaterally advanced osteoarthritis due to hip dysplasia, Tönnis grade III. Rotational acetabular osteotomy was performed on the right hip. (B) Seventeen-year postoperative follow-up radiograph shows a well restored joint space and no progression of osteoarthritis.

Figure 13 (A) Preoperative radiographs show decreased lateral center-edge angle (CEA), severe joint space narrowing and superolateral subluxation of the femoral head. (B) Periacetabular rotational osteotomy was performed and postoperative radiographs show increased lateral CEA, slightly restored joint space, reduced femoral head, excellent bony contact between acetabular fragment and pelvis.

Figure 14 Bernese periacetabular osteotomy. (A) External surface. (B) Internal surface. GM, gluteus medius tubercle; SM, sartorius muscle attachment; RFM, rectus femoris muscle (direct and indirect) heads.

Figure 15 Kirshner wire (K-wire) or Steinmann pin is inserted as a guide at the middle of the superior acetabular rim at the proposed level and angle.

Figure 16 Line of osteotomy which is marked by multiple drill holes.
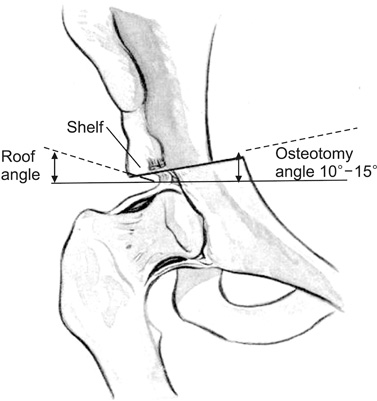
Figure 17 Ideal level of osteotomy is just above the capsular attachment between the capsule and the reflected head of rectus femoris. Osteotomy angle is the angle between the plane of the pelvic osteotomy and the horizontal plane (10°–15° upward and medially). Roof angle is the angle formed between the horizontal plane and a line joining the original outer acetabular lip to the new acetabular lip.
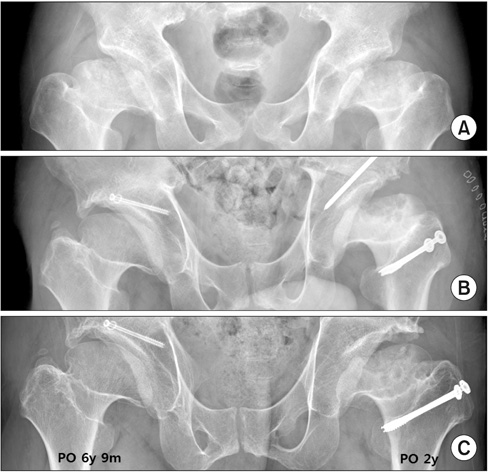
Figure 18 (A) Preoperative both hip anteroposterior (AP) radiograph of a 32-year-old man shows bilateral deformed femoral head with huge subchondral cyst due to multiple epiphyseal dysplasia. (B) Chiari osteotomy was performed. (C) Both hip AP radiograph taken at 6 years and 9 months (right hip), and at 2 years (left hip) after the operation show complete healing of subchondral cyst of the right femoral head.
Reference
-
1. Solomon L, Schnitzler CM. Pathogenetic types of coxarthrosis and implications for treatment. Arch Orthop Trauma Surg. 1983; 101:259–261.
Article2. Stulberg SD. Unrecognized childhood hip disease: a major cause of idiopathic osteoarthritis of the hip. In : Cordell LD, Harris WH, Ramsey PL, MacEwen GD, editors. The hip: Proceedings of the Third Open Scientific Meeting of the Hip Society. St. Louis (MO): CV Mosby;1975. p. 212–228.3. Cooperman DR, Wallensten R, Stulberg SD. Post-reduction avascular necrosis in congenital dislocation of the hip. J Bone Joint Surg Am. 1980; 62:247–258.
Article4. Cooperman DR, Wallensten R, Stulberg SD. Acetabular dysplasia in the adult. Clin Orthop Relat Res. 1983; (175):79–85.
Article5. Klaue K, Durnin CW, Ganz R. The acetabular rim syndrome. A clinical presentation of dysplasia of the hip. J Bone Joint Surg Br. 1991; 73:423–429.
Article6. Dorrell JH, Catterall A. The torn acetabular labrum. J Bone Joint Surg Br. 1986; 68:400–403.
Article7. Harris WH. Etiology of osteoarthritis of the hip. Clin Orthop Relat Res. 1986; (213):20–33.8. Millis MB, Murphy SB, Poss R. Osteotomies about the hip for the prevention and treatment of osteoarthrosis. J Bone Joint Surg. 1995; 77:626–647.
Article9. Ninomiya S, Tagawa H. Rotational acetabular osteotomy for the dysplastic hip. J Bone Joint Surg Am. 1984; 66:430–436.
Article10. Hasegawa Y, Iwase T, Kitamura S, Yamauchi Ki K, Sakano S, Iwata H. Eccentric rotational acetabular osteotomy for acetabular dysplasia: follow-up of one hundred and thirty-two hips for five to ten years. J Bone Joint Surg Am. 2002; 84:404–410.11. Kim HJ, Kim JW. Acetabular osteotomy. J Korean Hip Soc. 2004; 16:254–260.12. Ko JY, Wang CJ, Lin CF, Shih CH. Periacetabular osteotomy through a modified ollier transtrochanteric approach for treatment of painful dysplastic hips. J Bone Joint Surg Am. 2002; 84:1594–1604.
Article13. Nakamura S, Ninomiya S, Takatori Y, Morimoto S, Umeyama T. Long-term outcome of rotational acetabular osteotomy: 145 hips followed for 10-23 years. Acta Orthop Scand. 1998; 69:259–265.
Article14. Yasunaga Y, Ochi M, Terayama H, Tanaka R, Yamasaki T, Ishii Y. Rotational acetabular osteotomy for advanced osteoarthritis secondary to dysplasia of the hip. J Bone Joint Surg Am. 2006; 88:1915–1919.
Article15. Kang CS. Rotational acetabular osteotomy in acetabular dysplasia. J Korean Hip Soc. 2001; 13:208–213.
Article16. Kang CS, Shon SW, Kim SY. Rotational acetabular osteotomy for the dysplastic acetabulum. J Korean Orthop Assoc. 1986; 21:791–798.
Article17. Min BW, Bae KC, Kang CH, Song KS, Sohn SW. Rotational acetabular osteotomy for the dysplastic hip: a follow-up for 5 to 18 years. J Korean Orthop Assoc. 2005; 40:712–722.
Article18. Yoo MC, Cho YJ, Kim KI, Park HC, Jung CJ. Periacetabular rotational osteotomy in hip dysplasia: short term follow up result. J Korean Orthop Assoc. 2005; 40:434–441.
Article19. Hasegawa Y, Iwase T, Kitamura S, Kawasaki M, Yamaguchi J. Eccentric rotational acetabular osteotomy for acetabular dysplasia and osteoarthritis: follow-up at a mean duration of twenty years. J Bone Joint Surg Am. 2014; 96:1975–1982.20. Yasunaga Y, Fujii J, Tanaka R, et al. Rotational acetabular osteotomy. Clin Orthop Surg. 2017; 9:129–135.
Article21. Yasunaga Y, Takahashi K, Ochi M, et al. Rotational acetabular osteotomy in patients forty-six years of age or older: comparison with younger patients. J Bone Joint Surg Am. 2003; 85:266–272.22. Chang JS, Park JH, Park HG, Lee SH, Kim YK. Bernese periacetabular osteotomy for the hip dysplasia. J Korean Hip Soc. 1998; 10:141–148.23. Chang JS, Kwon KD, Shon HC. Bernese periacetbular osteotomy using dual approaches for hip dysplasia. J Korean Orthop Assoc. 2002; 37:226–232.24. Hussell JG, Rodriguez JA, Ganz R. Technical complications of the Bernese periacetabular osteotomy. Clin Orthop Relat Res. 1999; (363):81–92.
Article25. Myers SR, Eijer H, Ganz R. Anterior femoroacetabular impingement after periacetabular osteotomy. Clin Orthop Relat Res. 1999; (363):93–99.
Article26. Siebenrock KA, Leunig M, Ganz R. Periacetabular osteotomy: the Bernese experience. Instr Course Lect. 2001; 50:239–245.
Article27. Siebenrock KA, Schöll E, Lottenbach M, Ganz R. Bernese periacetabular osteotomy. Clin Orthop Relat Res. 1999; (363):9–20.
Article28. Steppacher SD, Tannast M, Ganz R, Siebenrock KA. Mean 20-year followup of Bernese periacetabular osteotomy. Clin Orthop Relat Res. 2008; 466:1633–1644.
Article29. Chiari K. Results of pelvic osteotomy as of the shelf method acetabular roof plastic. Z Orthop Ihre Grenzgeb. 1955; 87:14–26.30. White RE Jr, Sherman FC. The hip-shelf procedure. A long-term evaluation. J Bone Joint Surg Am. 1980; 62:928–932.
Article31. Park YS. Chiari pelvic osteotomy. J Korean Hip Soc. 2001; 13:214–216.32. Graham S, Westin GW, Dawson E, Oppenheim WL. The Chiari osteotomy. A review of 58 cases. Clin Orthop Relat Res. 1986; (208):249–258.33. Kawamura B, Hosono S, Yokogushi K. Dome osteotomy of the pelvis. In : Tachdjian MO, editor. Congenital dislocation of the hip. New York: Churchill-Livingstone;1982. p. 609–623.34. Matsuno T, Ichioka Y, Kaneda K. Modified Chiari pelvic osteotomy: a long-term follow-up study. J Bone Joint Surg Am. 1992; 74:470–478.35. Chiari K. Medial displacement osteotomy of the pelvis. Clin Orthop Relat Res. 1974; (98):55–71.
Article36. Anwar MM, Sugano N, Matsui M, Takaoka K, Ono K. Dome osteotomy of the pelvis for osteoarthritis secondary to hip dysplasia. An over five-year follow-up study. J Bone Joint Surg Br. 1993; 75:222–227.
Article37. Nakata K, Masuhara K, Sugano N, Sakai T, Haraguchi K, Ohzono K. Dome (modified Chiari) pelvic osteotomy: 10- to 18-year followup study. Clin Orthop Relat Res. 2001; (389):102–112.38. Kotz R, Chiari C, Hofstaetter JG, Lunzer A, Peloschek P. Long-term experience with Chiari's osteotomy. Clin Orthop Relat Res. 2009; 467:2215–2220.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Use of Xenograft ( Lubboc(r)) for Pelvic Osteotomy in Children
- Osteotomies Around the Hip Joint
- Triple Osteotomy of the Innominate Bone: Experlence with an adult Paralytie Hip
- Chiari Pelvic Osteotomy in Children and Adolescent
- 20-Year-Follow up of Treatment Using Spine Osteotomy and Halo-pelvic Traction for Tuberculous Kyphosis: A Case Report
