Clinical Usage of Ultrasonography for the Hip Joint
- Affiliations
-
- 1Department of Orthopedic Surgery, Keimyung University School of Medicine, Daegu, Korea. oslee@dsmc.or.kr
- KMID: 2421341
- DOI: http://doi.org/10.4055/jkoa.2017.52.6.476
Abstract
- Thorough history taking and physical examination are highly important for the correct diagnosis of hip disease, and several diagnostic imaging tools are available depending on suspected diseases. Recently, the clinical use of ultrasonography has been increasing due to its relatively low cost, less invasiveness, and the possibility for dynamic evaluation. The purpose of this article was to review the basic technique and normal anatomic images for the clinical usage of ultrasonography around the hip joint and describe typical ultrasonographic findings of several hip diseases.
Keyword
Figure
-

Figure 1 Anterior hip longitudinal axis. (A) Position of transducer (along the femoral neck). (B) Ultrasonography shows intact anterior capsule (block arrow) and collapsed synovial recess (arrows). FH, femoral head.
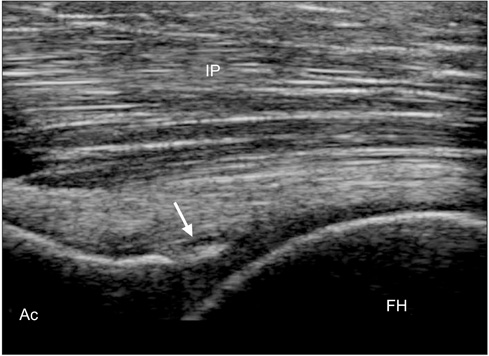
Figure 2 Sagittal plane ultrasonography of the anterior hip joint shows intact hyperechoic triangular labrum (arrow). IP, iliopsoas; Ac, acetabulum; FH, femoral head.

Figure 3 Transverse plane ultrasonography of the ASIS level. Tendon lies behind the IP muscle (arrows). Block arrow indicates iliopsoas tendon. IP, iliopsoas; ASIS, anterior-superior iliac spine.
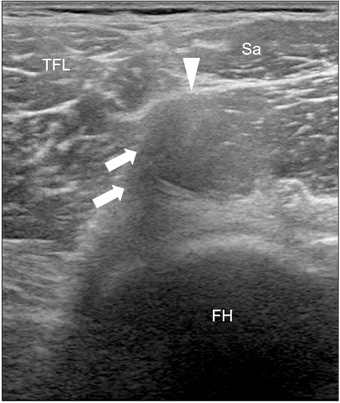
Figure 4 Transverse plane ultrasonography of the anterior-inferior iliac spine level. White arrows indicate acoustic shadowing due to the obliquity of indirect head of the rectus femoris compared with the direct head of the muscle (arrowhead). TFL, tensor fascia lata; Sa, sartorius; FH, femoral head.
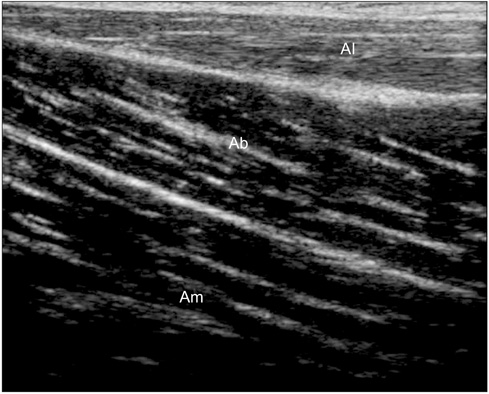
Figure 5 Medial hip longitudinal axis ultrasonography shows a three layer of the adductor muscle. These muscles are divided by hyperechoic fascial planes. Al, adductor longus; Ab, adductor brevis; Am, adductor magnus.
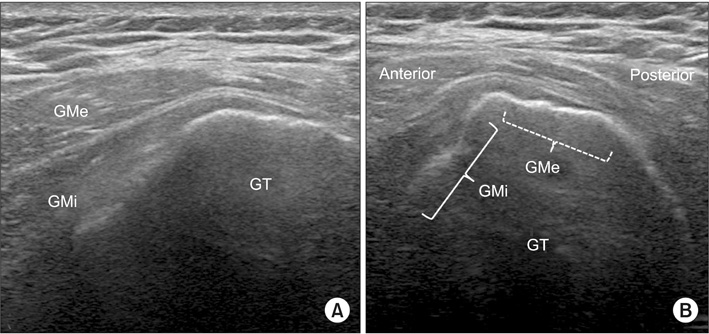
Figure 6 Lateral hip ultrasonography. (A) Longitudinal axis. (B) Transverse axis. GMe, gluteus medius; GMi, gluteus minimus; GT, greater trochanter.
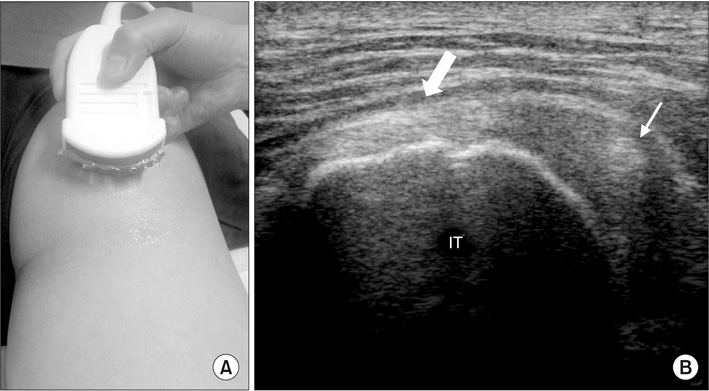
Figure 7 Posterior hip ultrasonography. (A) Convex transducer can be useful for posterior examination. (B) Transverse scan around the IT. Block arrow indicates conjoined tendon of the hamstring muscle, and arrow indicates sciatic nerve that is located just lateral to IT. IT, ischial tuberosity.
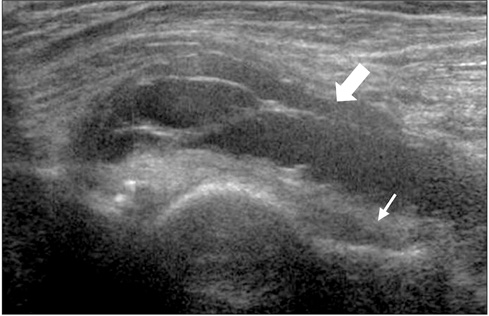
Figure 8 Anterior hip ultrasonography shows distended iliopsoas bursa (block arrow) and anterior synovial recess (arrow).
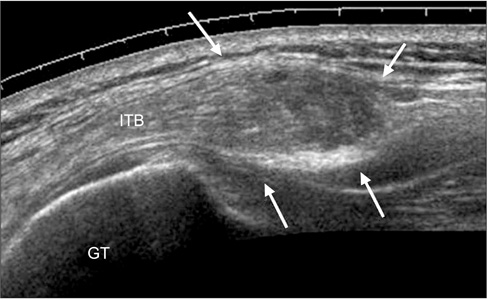
Figure 9 Lateral hip ultrasonography shows hypertrophied ITB (arrows) over the GT. ITB, iliotibial band; GT, greater trochanter.
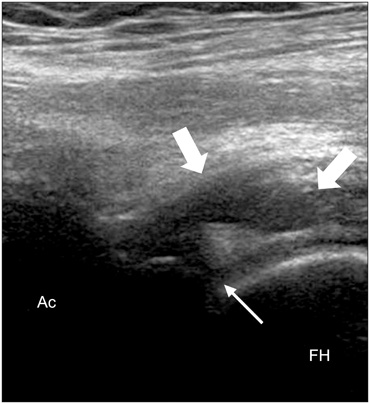
Figure 10 Anterior hip ultrasonography shows detached anterolateral labrum from the bony Ac (arrow). Para-labral cyst is also shown along the tear (block arrows). Ac, acetabulum; FH, femoral head.
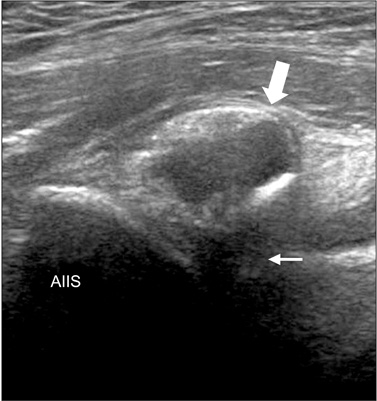
Figure 11 Anterior hip ultrasonography shows calcification in the rectus femoris (block arrow). Acoustic shadowing is also shown beneath the calcification (arrow). AIIS, anterior inferior iliac spine.

Figure 12 Posterior hip ultrasonography shows large cystic mass (bursitis) around the IT (arrow). IT, ischial tuberosity.
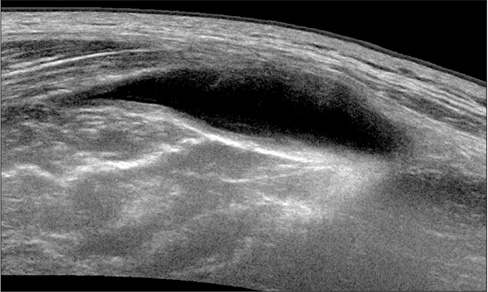
Figure 13 Lateral hip ultrasonography shows distension of the bursa beneath gluteus maximus, around the greater trochanter.

Figure 14 Photographs showing an image of ultrasonography of the gluteal muscle detachment (A) and intraoperative findings (B). GMe, gluteus medius; GMi, gluteus minimus; GT, greater trochanter.
Reference
-
1. Cardinal E, Beauregard CG, Chhem RK. Interventional musculoskeletal ultrasound. Semin Musculoskelet Radiol. 1997; 1:311–318.
Article2. Dodd GD 3rd, Esola CC, Memel DS, et al. Sonography: the undiscovered jewel of interventional radiology. Radiographics. 1996; 16:1271–1288.
Article3. Rubens DJ, Fultz PJ, Gottlieb RH, Rubin SJ. Effective ultrasonographically guided intervention for diagnosis of musculoskeletal lesions. J Ultrasound Med. 1997; 16:831–842.
Article4. Baffroy-Fayard N. Groupe de travail du CCLIN Paris-Nord. Infection control in interventional radiology: good practice guideline. J Radiol. 2002; 83:351–359.5. Nam WD, Nam SW, Han KY. Ultrasonographic findings of normal hip joint and painful hip due to soft tissue problem. J Korean Orthop Ultrasound Soc. 2010; 3:38–46.6. Louis LJ. Musculoskeletal ultrasound intervention: principles and advances. Radiol Clin North Am. 2008; 46:515–533.
Article7. Rowbotham EL, Grainger AJ. Ultrasound-guided intervention around the hip joint. AJR AM J Roentgenol. 2011; 197:122–127.
Article8. Chu CR, Coyle CH, Chu CT, et al. In vivo effects of single intra-articular injection of 0.5% bupivacaine on articular cartilage. J Bone Joint Surg Am. 2010; 92:599–608.
Article9. Saker MB, Kane RA, Matalon TAS. Factors affecting and techniques to improve needle visualization. Semin Interv Radiol. 1997; 14:471–475.
Article10. Chan YL, Cheng JC, Metreweli C. Sonographic evaluation of hip effusion in children. Improved visualization with the hip in extension and abduction. Acta Radiol. 1997; 38:867–869.11. Robben SG, Lequin MH, Diepstraten AF, den Hollander JC, Entius CA, Meradji M. Anterior joint capsule of the normal hip and in children with transient synovitis: US study with anatomic and histologic correlation. Radiology. 1999; 210:499–507.
Article12. Moss SG, Schweitzer ME, Jacobson JA, et al. Hip joint fluid: detection and distribution at MR imaging and US with cadaveric correlation. Radiology. 1998; 208:43–48.
Article13. Han KY. Painful causes around hip joint and evaluation using ultrasonography. J Korean Orthop Ultrasound Soc. 2009; 2:45–52.14. Karpinski MR, Piggott H. Greater trochanteric pain syndrome. A report of 15 cases. J Bone Joint Surg Br. 1985; 67:762–763.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Application of the Ultrasound in Painful Pediatric Hip
- A Case of Gouty Arthritis Involving the Hip Joint Diagnosed Using Ultrasonography
- Clinical Significance of Ultrasonography for Detection of Hip Joint Effusion in Children: Analysis of the 23 Cases of Transient Synovitis of the Hip
- An ultrasonographic study on measurement of normal hip joint in Korean
- Suppurative Arthritis of the Hip Joint in Coma Patient: Two Cases
