Tracheobronchial Branching Anomalies
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University Cheonan Hospital, Korea. ytokim@schca.ac.kr
- 2Department of Family Medicine, Soonchunhyang University Hospital, Korea.
Abstract
- There are various congenital anomalies with respect to the number, length, diameter, and location of tracheobronchial branching patterns. The tracheobronchial anomalies are classified into two groups. The first one, anomalies of division, includes tracheal bronchus, cardiac bronchus, tracheal diverticulum, pulmonary isomerism, and minor variations. The second one, dysmorphic lung, includes lung agenesis-hypoplasia complex and lobar agenesis-aplasia complex.
MeSH Terms
Figure
-

Fig. 1 Three major theories of congenital bronchial anomaly. A. Reduction theory. Perforated lines mean major potential abnormal bronchial patterns. These abnormal bronchi shrink during embryologic development normally. The persistence of such bronchi results in a tracheal diverticulum or a tracheal bronchus or a cardiac bronchus. B. Migration theory. Right upper lobe bronchus (RUL br) has migrated from its hyparterial location to eparterial location on the right main bronchus. C. Selection theory. The interaction has happened between bronchial epithelium and bronchial mesenchyme (gray area demarcated by perforated lines). The tracheal epithelium is protected by tracheal mesenchyme (black line) originally. But there may be epithelial budding on a weak point of tracheal mesenchyme due to epitheliomesenchymal interaction and abnormal organogenesis. A right tracheal bronchus (Rt TB) is an example. PA = pulmonary artery, LLL br = left lower lobe bronchus, Lt TB = left tracheal bronchus, Rt TB = right tracheal bronchus, LUL br = left upper lobe bronchus, ML br = middle lobe bronchus, RLL br = right lower lobe bronchus, Rt TB = right tracheal bronchus, RULB = right upper lobe bronchus. AC br = accessory cardiac bronchus.

Fig. 2 Tracheal bronchus: An anomalous bronchus from lower trachea. A. Axial scan shows an anomalous bronchus (arrow) from the right lateral wall of lower trachea, which supply the apical segment of right upper lobe. B. Reformatted coronal images demonstrates the small tracheal bronchus (arrow) and right upper bronchus normally arising from the right main bronchus (arrowhead).

Fig. 3 Tracheal bronchus: An anomalous bronchus from lower trachea. Serial axial images show a small anomalous bronchus (white arrow) from lower trachea, which supply some portion of apical segment of right upper lobe. And also note apical (open arrowhead), anterior (black arrow) and posterior (arrowhead) segmental bronchi arising from the right upper lobe bronchus.
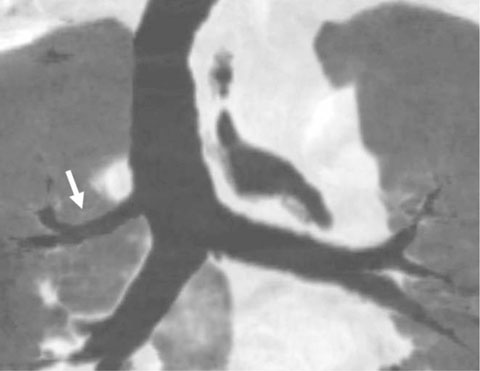
Fig. 4 Tracheal bronchus: Right upper lobe bronchus from lower trachea. Coronal thin-slab MinIP image shows the right upper lobe bronchus (arrow) arising from the trachea 1 cm proximal to the carina. It is called as "pig bronchus".
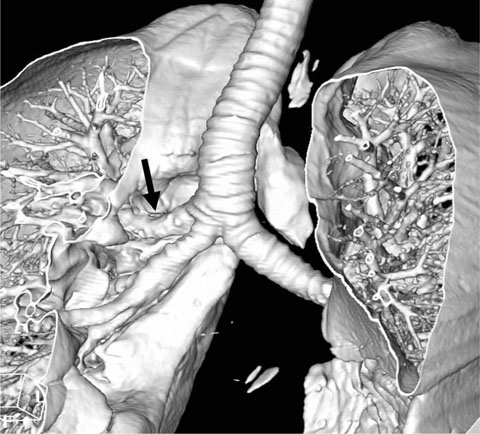
Fig. 5 Tracheal bronchus: Right upper lobe bronchus from tracheal bifurcation. Volume rendered image shows that the right upper lobe bronchus (arrow) arising from the trachea near the bifurcation site, instead of normal position.

Fig. 6 Tracheal bronchus: Double right upper lobe bronchi from right main bronchus. Volume rendered image shows two right upper lobe bronchi (arrow, arrowhead) arising from the right main bronchus.

Fig. 7 Tracheal bronchus: Postepartrial right upper lobe bronchus. A. B. Axial (A) and reformatted coronal image (B) show the right upper lobe bronchus (arrow) arising posterior to and at the same level of the right pulmonary artery (open arrow), described as posteparterial. Normally, the right main bronchus is eparterial as arising above right pulmonary artery. Postepaterial right upper lobe bronchus is included in the wide spectrum of tracheal bronchus.

Fig. 8 Cardiac bronchus. Reformed volume rendered image clearly shows a diverticulum (arrow) with blind pouch, arising from the medial wall of the bronchus intermedius.

Fig. 9 Cardiac bronchus with own accessary lobe. A, B. Axial (A) and reformatted coronal images (B) show an accessory cardiac bronchus (arrow) that originates from the medial aspect of the right bronchus intermedius. There is an anomalous accessory lobe (*) with apparent pleural fissure (arrowhead), separating from right lower lobe.

Fig. 10 Cardiac bronchus with own accessory lobe. A 43-year-old man has complained of cough and sputum. A. Axial scan with lung setting shows cardiac bronchus (arrowhead) and bronchiolitis in right lower lobe. B. Axial scan shows accessary lobe with increased attenuation (arrow), suggesting combined infection.

Fig. 11 Tracheal diverticulum. Axial image shows a round outpouching (arrow) from the right posterior-lateral wall of the trachea.

Fig. 12 Tracheal diverticulum. Volume rendered image shows a round outpouching (arrow) from the right posterior-lateral wall of the trachea.

Fig. 13 Left isomerism with heterotaxy syndrome in a 34-year-old man. A. Axial image demonstrates morphologically similating both atria (*). B. Coronal thin-slab MinIP image shows bilateral main bronchus with bilobar branching pattern. PA= pulmonary artery.

Fig. 14 Supernumery bronchus to the superior segment of the right lower lobe. Serial Axial images reveal a superior and medial subsegmental bronchus (black arrow) of superior segment of right lower lobe. A lateral subsegmental bronchus (white arrow) originates separately.

Fig. 15 Supernumery bronchus to the superior segment of the right lower lobe. A. Serial axial images show a small bronchus (arrowhead) supplying superior subsegment of superior segment of right lower lobe. And also note the main portion of the superior segment bronchus (arrow) at the level of right middle lobe. B. Reformatted slap minIP image shows two bronchi (arrowhead, arrow) supplying superior segment of right lower lobe.

Fig. 16 Medial basal segmental bronchus of left lower lobe: an independent origin. Serial axial images show medial basal bronchus (arrow) arising from left lower lobe basal bronchus independently. Normally, the medial and anterior basal bronchi originate together as a common trunk.

Fig. 17 Supranumery bronchus from right middle lobe bronchus. Serial axial images shows an anomalous bronchus (white arrow) arising from inferior portion of right middle lobe bronchus (black arrow), which traverses the minor fissure to medial basal segment of right lower lobe.
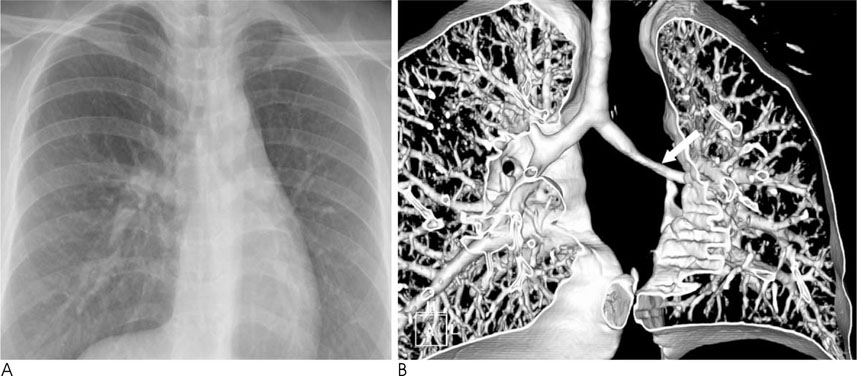
Fig. 18 Agenesis of left upper lobe in a 35-year-old woman. A. Chest radiograph shows slightly decreased left lung volume with mediastinal shifting. B. Volume rendered image shows the absence of the left upper lobe bronchus (arrow: normal origin site of left upper lobe bronchus) from main bronchus, and small left lung with the mediastinal shift to the left side.

Fig. 19 Scimitar syndrome in a 56-year-old woman. A. Volume rendered image shows scimitar vein (open arrowheads) in the right lung. B. Serial axial images show anomalous fissure (arrows), separating medial and lateral portion of right lung. Also note scimitar vein (arrowheads) near the anomalous fissure. C. Coronal thin-slab minIP image shows anomalous branching of right bronchi.
Reference
-
1. Yedururi S, Guillerman RP, Chung T, Braverman RM, Dishop MK, Giannoni CM, et al. Multimodality imaging of tracheobronchial disorders in children. Radiographics. 2008; 28:E29.2. Ghaye B, Szapiro D, Fanchamps JM, Dondelinger RF. Congenital bronchial abnormalities revisited. Radiographics. 2001; 21:105–119.3. Beigelman C, Howarth NR, Chartrand-Lefebvre C, Grenier P. Congenital anomalies of tracheobronchial branching patterns: spiral CT aspects in adults. Eur Radiol. 1998; 8:79–85.4. Zylak CJ, Eyler WR, Spizarny DL, Stone CH. Developmental lung anomalies in the adult: radiologic-pathologic correlation. Radiographics. 2002; S25–S43.5. Goo JM, Im JG, Ahn JM, Moon WK, Chung JW, Park JH, Seo JB, Han MC. Right paratracheal air cysts in the thoracic inlet: clinical and radiologic significance. AJR Am J Roentgenol. 1999; 173:65–70.6. Soto-Hurtado EJ, Peñuela-Ruíz L, Rivera-Sánchez I, Torres-Jiménez J. Tracheal diverticulum: a review of the literature. Lung. 2006; 184:303–307.7. Applegate KE, Goske MJ, Pierce G, Murphy D. Situs revisited: imaging of the heterotaxy syndrome. Radiographics. 1999; 19:837–852.8. Mata JM, Cáceres J. The dysmorphic lung: imaging findings. Eur Radiol. 1996; 6:403–414.9. Godwin JD, Tarver RD. Scimitar syndrome: four new cases examined with CT. Radiology. 1986; 159:15–20.10. Frank JL, Poole CA, Rosas G. Horseshoe lung: clinical, pathologic, and radiologic features and a new plain film finding. AJR Am J Roentgenol. 1986; 146:217–226.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Pulmonary Artery Sling Associated with Tracheobroncheal Hypoplasia
- Ruptured proximal anterior cerebral artery (A1) aneurysm located at an anomalous branching of the fronto-orbital artery--a case report
- Effect of Anesthetics on Protein Content of Alveolar Washings of Rabbits
- Esophageal stenosis due to tracheobronchial remnants: a case report
- Usefulness of intraoperative bronchoscopy during surgical repair of a congenital cardiac anomaly with possible airway obstruction: three cases report
