Ann Dermatol.
2018 Oct;30(5):624-626. 10.5021/ad.2018.30.5.624.
A Case of Abortive Staphylococcal Scalded Skin Syndrome
- Affiliations
-
- 1Department of Dermatology, Kangnam Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea. dermap@hanmail.net, hyeonekim@gmail.com
- KMID: 2419760
- DOI: http://doi.org/10.5021/ad.2018.30.5.624
Abstract
- No abstract available.
MeSH Terms
Figure
-

Fig. 1 Diffuse erythroderma involves the neck, trunk, and extremities with sandpaper-like coarseness (A), and perioral crust and fissure (B) were observed. Several vesicobullae and erosive lesions were observed in the lower abdomen, without Nikolsky sign (C). The desquamation worsened and the erythema gradually faded on the 8th day after admission (D~F) (We received the patient's consent form about publishing all photographic materials).
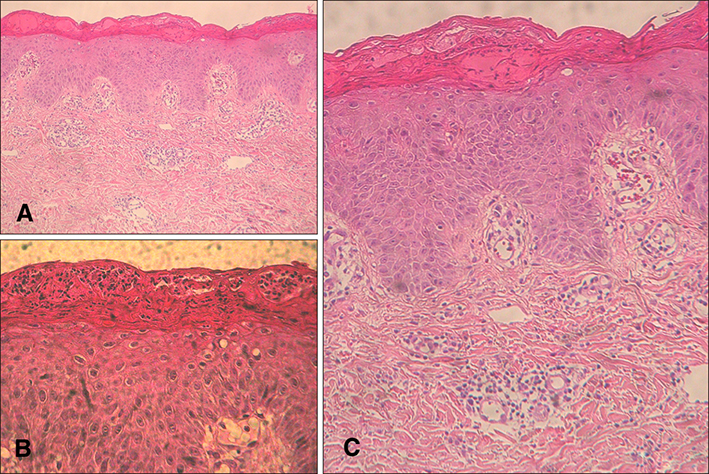
Fig. 2 In histology, neutrophils seen in the subcorneal lesion with mild perivascular lymphocytic infiltration were observed, but blistering was not distinct (H&E, A: ×40; B: ×200). Acantholysis was observed with little or scarce inflammatory cell infiltrate and no cell necrosis (C: H&E, ×100).
Reference
-
1. Park AY, Yeon EK, Lee HK, Shin MY. A clinical review of staphylococcal scalded skin syndrome for the last 10 years. Soonchunhyang Med Sci. 2012; 18:32–37.
Article2. Patel GK, Finlay AY. Staphylococcal scalded skin syndrome: diagnosis and management. Am J Clin Dermatol. 2003; 4:165–175.3. Ladhani S, Evans RW. Staphylococcal scalded skin syndrome. Arch Dis Child. 1998; 78:85–88.
Article4. Park JW, Hwang DK, Yu HJ. Staphylococcal scalded skin syndrome, review of 20 cases. Korean J Dermatol. 2002; 40:1051–1057.5. Kang JD, Park SD. Reclassification of staphylococcal scalded skin syndrome by clinical analysis of 25 cases. Korean J Dermatol. 2004; 42:398–405.
