Pulmonary Comorbidities of Lung Emphysema
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University College of Medicine, Cheonan Hospital, Cheonan, Korea. ytokim@schmc.ac.kr
- KMID: 2418655
- DOI: http://doi.org/10.3348/jksr.2018.79.3.139
Abstract
- Pulmonary emphysema is defined as the "abnormal permanent enlargement of the airspaces distal to the terminal bronchioles accompanied by destruction of the alveolar wall and without obvious fibrosis." Pulmonary emphysema could result in various complications or comorbidities, many of which are interrelated. Pulmonary emphysema can result in a number of interrelated complications and comorbidities. When pulmonary emphysema is accompanied by comorbidities, it may exhibit different and unique radiologic findings, depending on the underlying lung condition. The purpose of this article was to review radiologic findings that have been reported in patients with underlying emphysema, as well as localized pulmonary comorbidities including infection, fibrosis, primary lung cancer, hemorrhage, and other rare conditions.
MeSH Terms
Figure
-
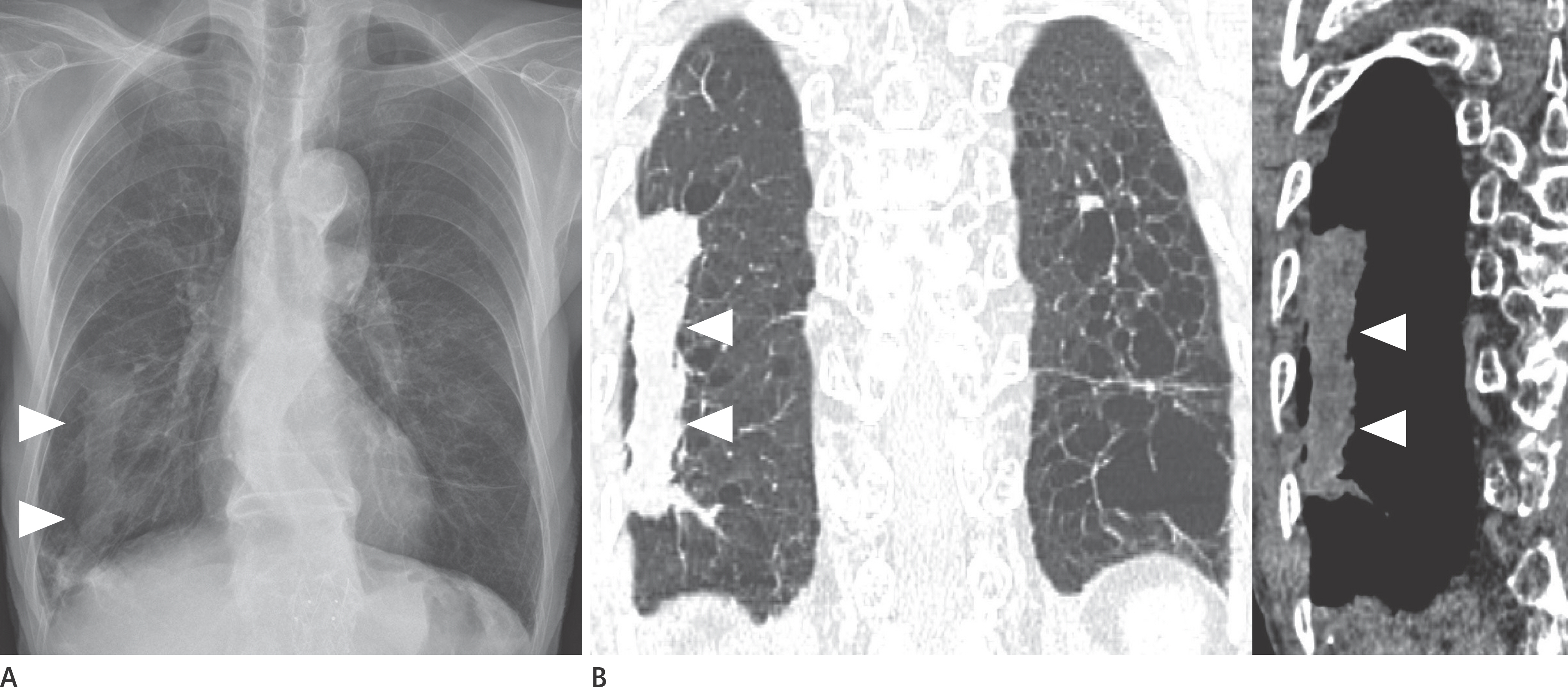
Fig. 1 Pneumonia with underlying emphysema in an 80-year-old man. A. Chest radiograph shows a long rectangular structure (arrowheads) in the right lower lung. B. Coronal CT images show a long rectangular mass-like lesion (arrowheads) in the right lower lobe. This was confirmed as chronic nonspecific pneumonitis by percutaneous transthoracic needle biopsy. Also note emphysema in both lungs. Pneumonia that develops in an emphysematous lung may manifest as an unusual finding.

Fig. 2 Pneumonia with underlying emphysema in a 79-year-old man. A. Chest radiograph shows irregular consolidation in the right upper lobe and irregular reticular or reticulo-nodular opacities in both lower lungs. B. CT shows ill-defined consolidation with multiple small, low-attenuation (Swiss cheese-like appearance) lesions in the right lung and left lower lobe. The reticular or reticulo-nodular opacities in both lower lungs on chest radiograph correspond to pneumonic consolidation with underlying emphysema on CT. Pneumonia that develops in an emphysematous lung may mimic interstitial lung disease.

Fig. 3 Pneumonia with underlying severe emphysema in an 84-year-old man. Axial and reformatted coronal CT images show multiple irregular cystic lesions containing fluid (asterisks) in the left lower lobe and severe emphysema in the right lung. Pulmonary infection that develops in severe emphysematous lung may mimic cystic lung disease.
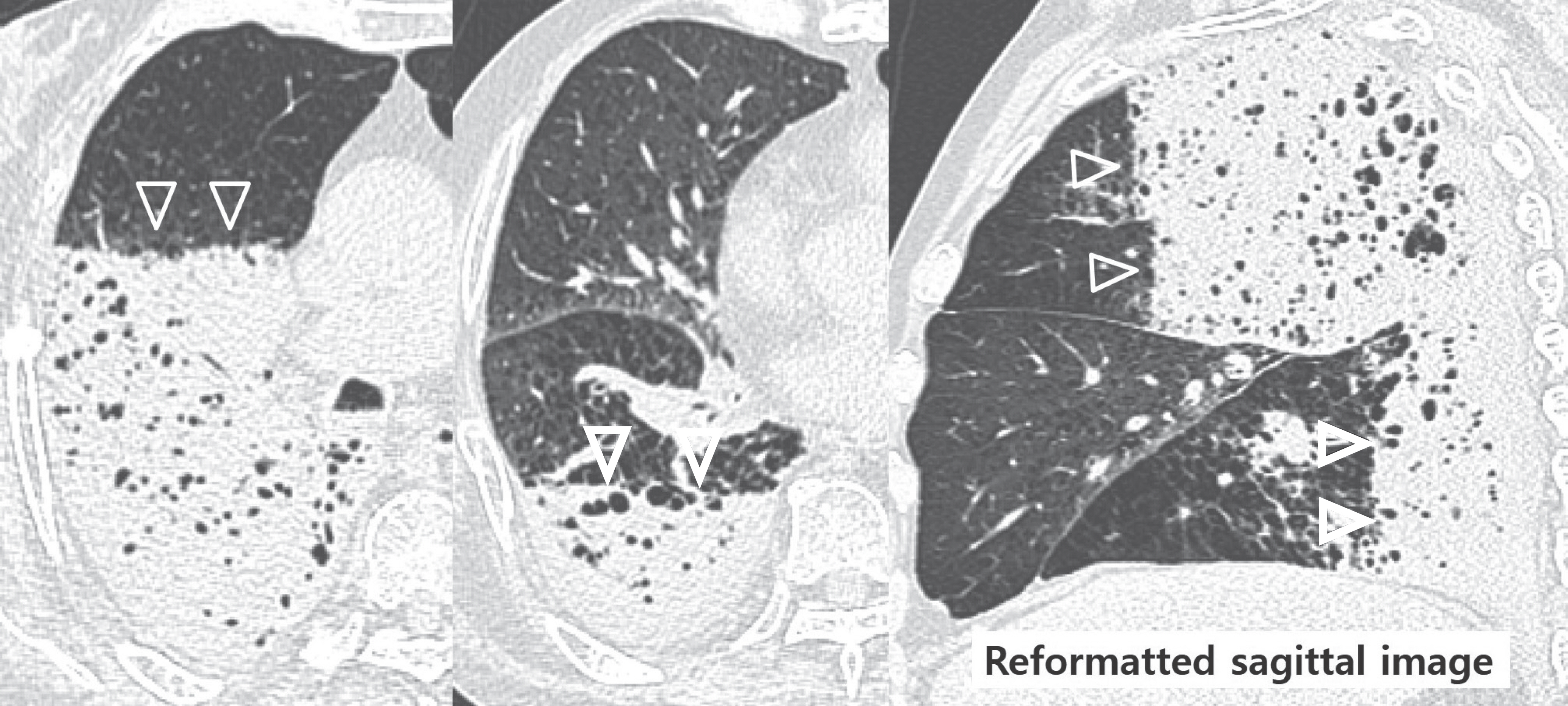
Fig. 4 Pneumonia with underlying emphysema in a 75-year-old man. Axial and sagittal images show horizontal fluid levels (arrowheads) between the consolidative lesion and the preserved lung in the right upper and lower lobes.
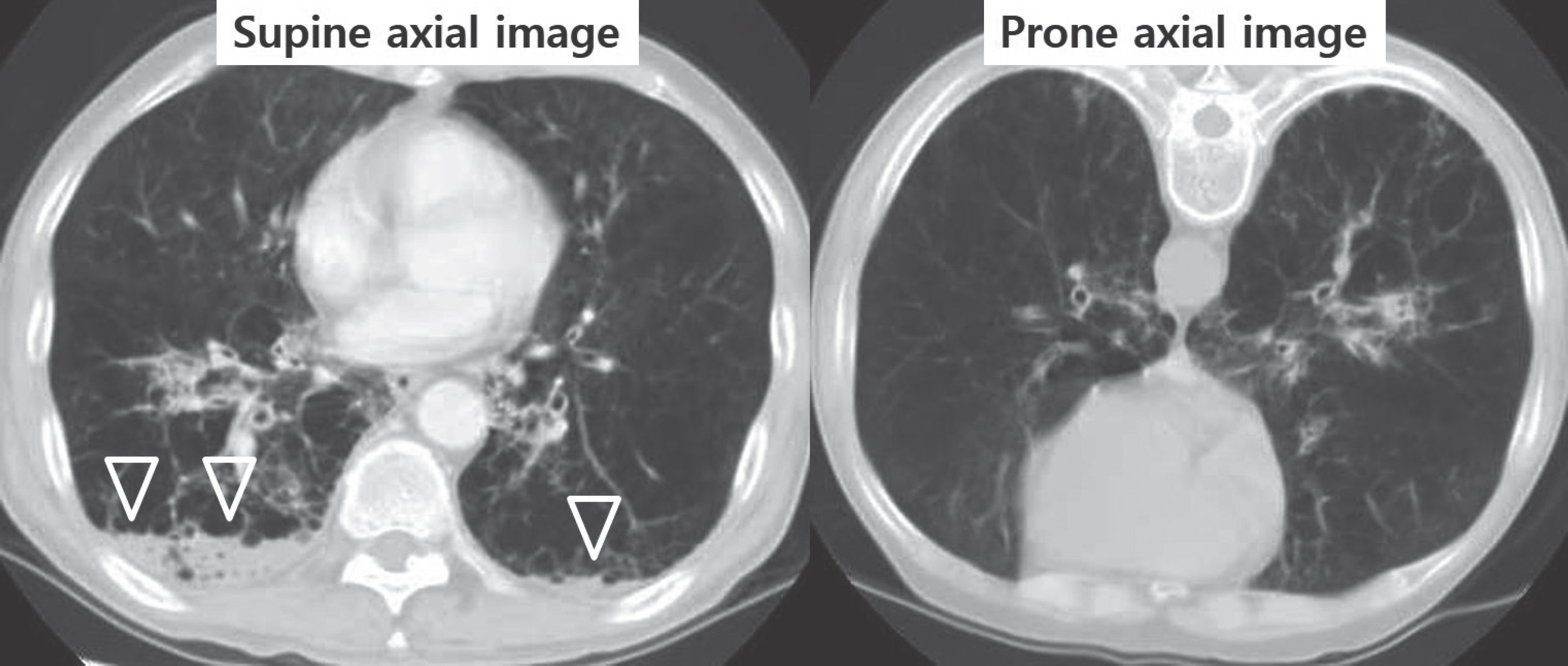
Fig. 5 Pneumonia with underlying emphysema in a 63-year-old man. Supine axial image shows fluid levels (arrowheads) in the dependent portion of both lower lobes. On prone axial image obtained the same day, fluid levels have disappeared.

Fig. 6 The sequential change in bulla by infection in a 64-year-old man. Initial CT image shows a bulla (arrow) at the right azygoesophageal recess. Follow-up CT image obtained 6 months later shows a mediastinal thin walled cystic lesion with air-fluid level (open arrow). A bulla is smaller and anteriorly displaced (arrow). On follow-up CT image obtained 18 months later, the mediastinal thin-walled cystic lesion has disappeared, although the bulla has persisted (arrow).
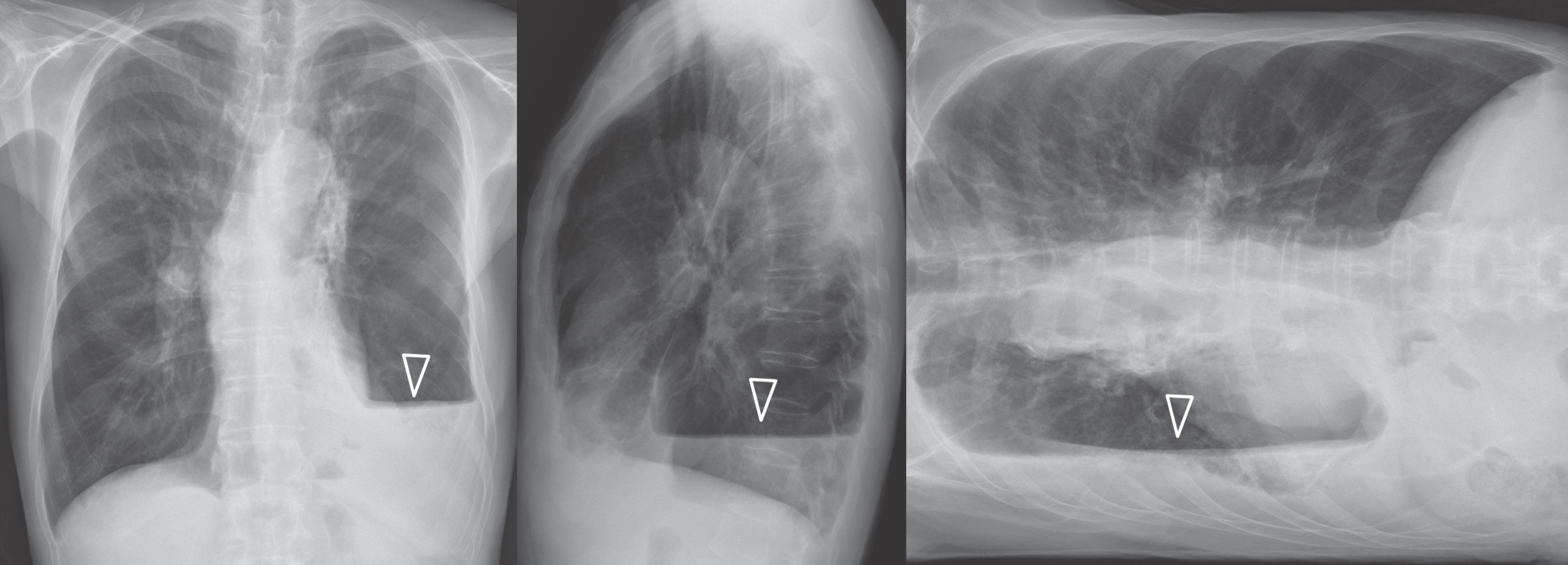
Fig. 7 Air fluid level in an infected bulla in the left lower lobe in a 63-year-old man. Chest posteroanterior and lateral views show air-fluid levels (arrowheads) in the dependent portion of both lower lobes.
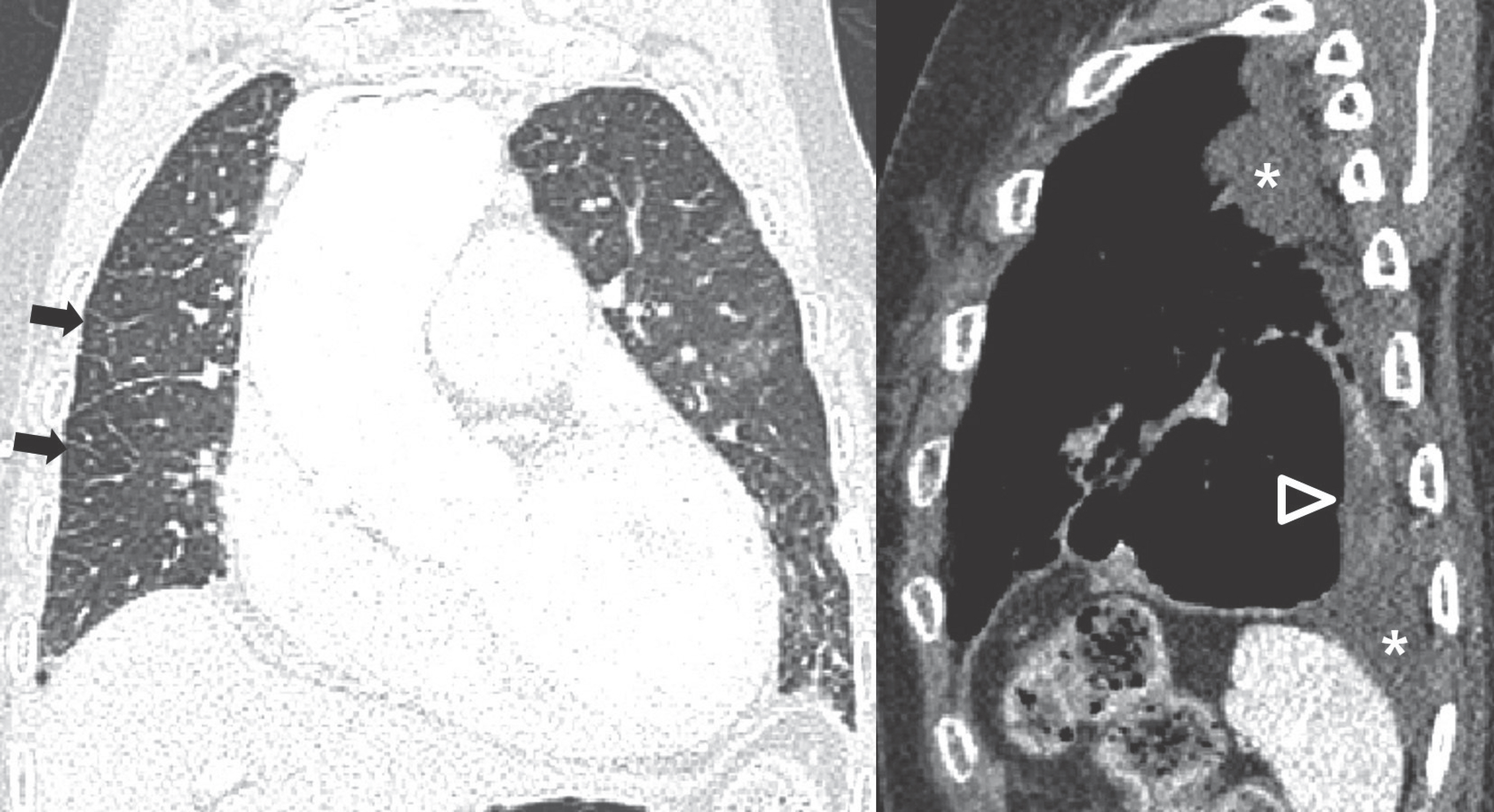
Fig. 8 Air fluid level in a bulla in a 90-year-old woman with pulmonary edema. Coronal CT image shows interlobular septal thickening in the right lung (arrows), suggesting pulmonary edema; also note cardiomegaly. Sagittal CT image shows air-fluid level in the bulla (arrowhead) in the left lower lobe; also note left pleural effusion (asterisk).
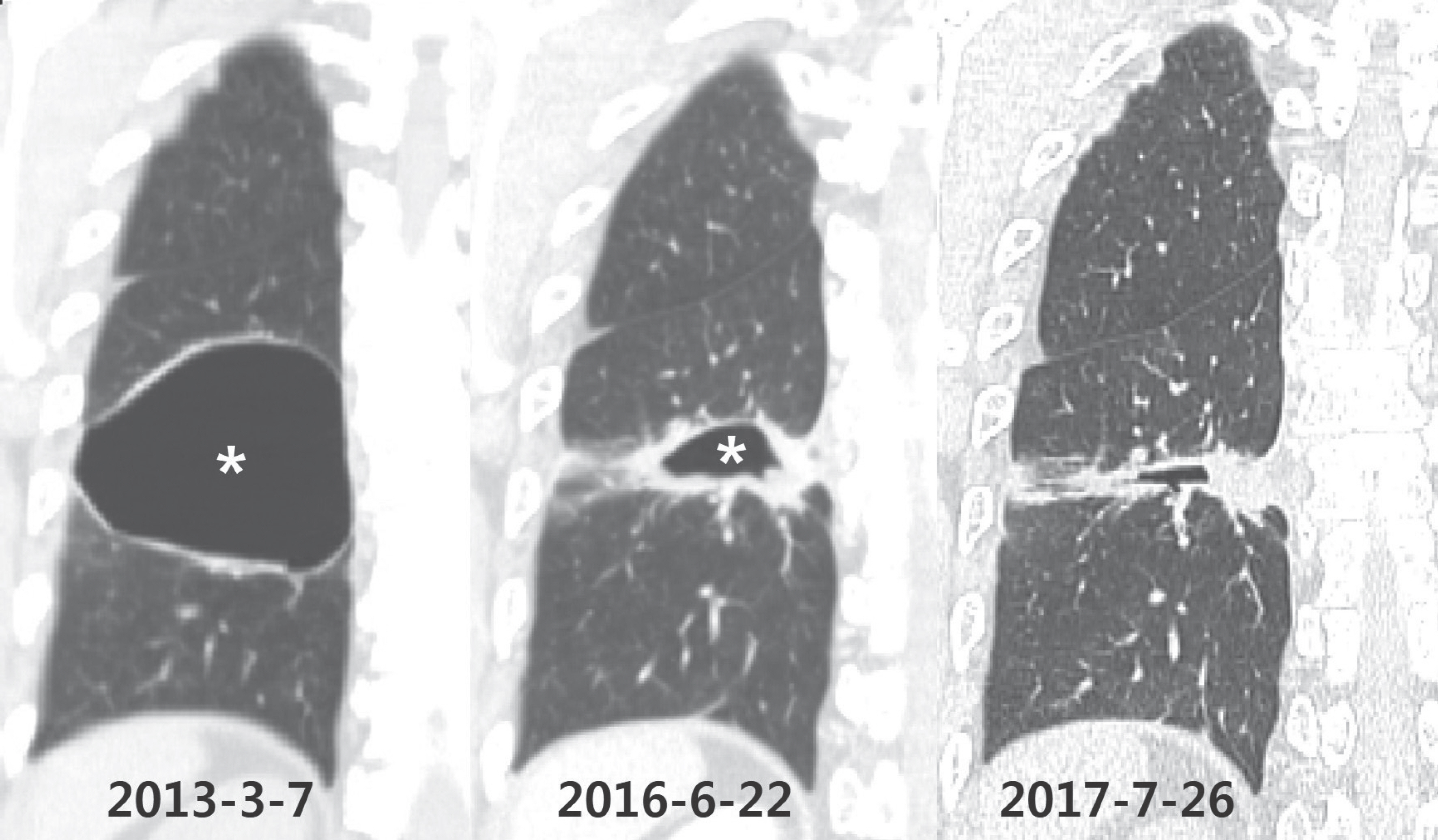
Fig. 9 Autobullectomy of a bulla by infection in a 61-year-old man. Initial coronal image shows a large bulla (asterisk) in the right lower lobe. On follow-up CT images, the bulla became smaller with an irregular thick wall. If initial CT image is unavailable, this needs to be differentiated from other cavitary disease such as tuberculosis.

Fig. 10 Autobullectomy by lung cancer in a 51-year-old man. A. Initial CT images shows lung cancer (asterisk) and multiple air fluid levels in bullae (arrowheads) in the right upper lobe. B. On CT images after 4 months, lung cancer (asterisk) is enlarged and the previously noted air-fluid level in the bulla of the right upper lobe has disappeared.
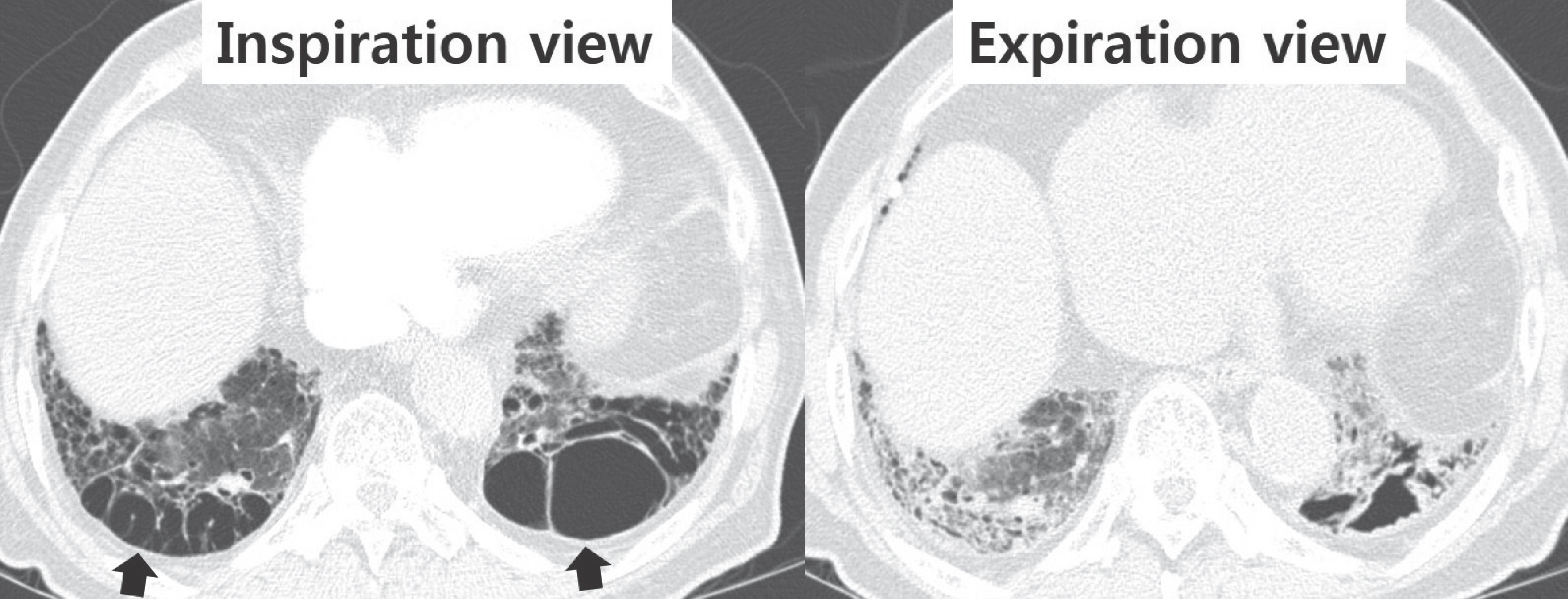
Fig. 11 Changes in bullae by degree of respiration in an 87-year-old man. Bullae (arrows) in both lower lobes have markedly decreased in expiration view.
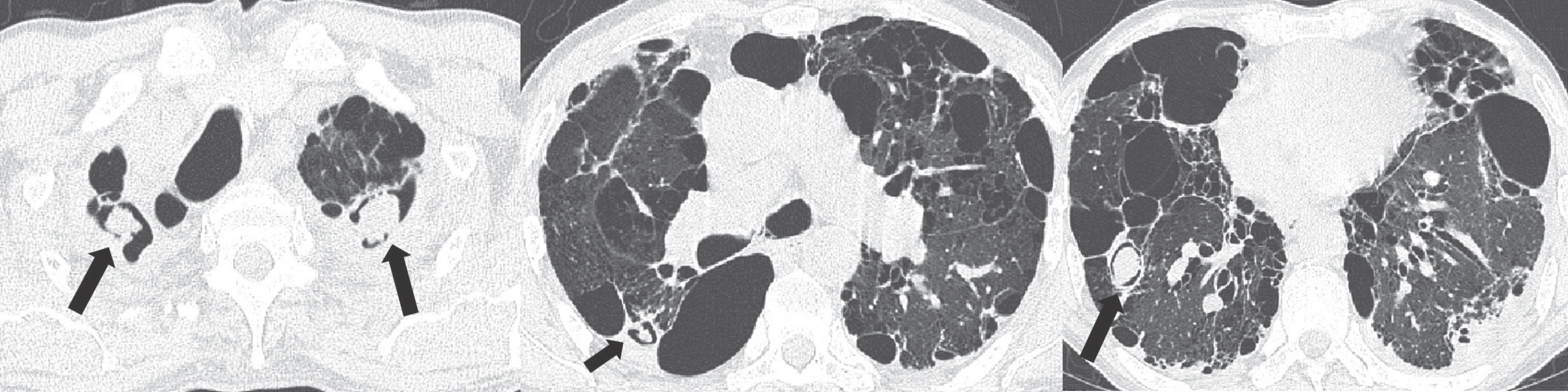
Fig. 12 Multiple aspergillomas in a bulla in a 59-year-old man. Serial axial images show multiple aspergillomas (arrows) with air crescent signs in the right lung and the left upper lobe.
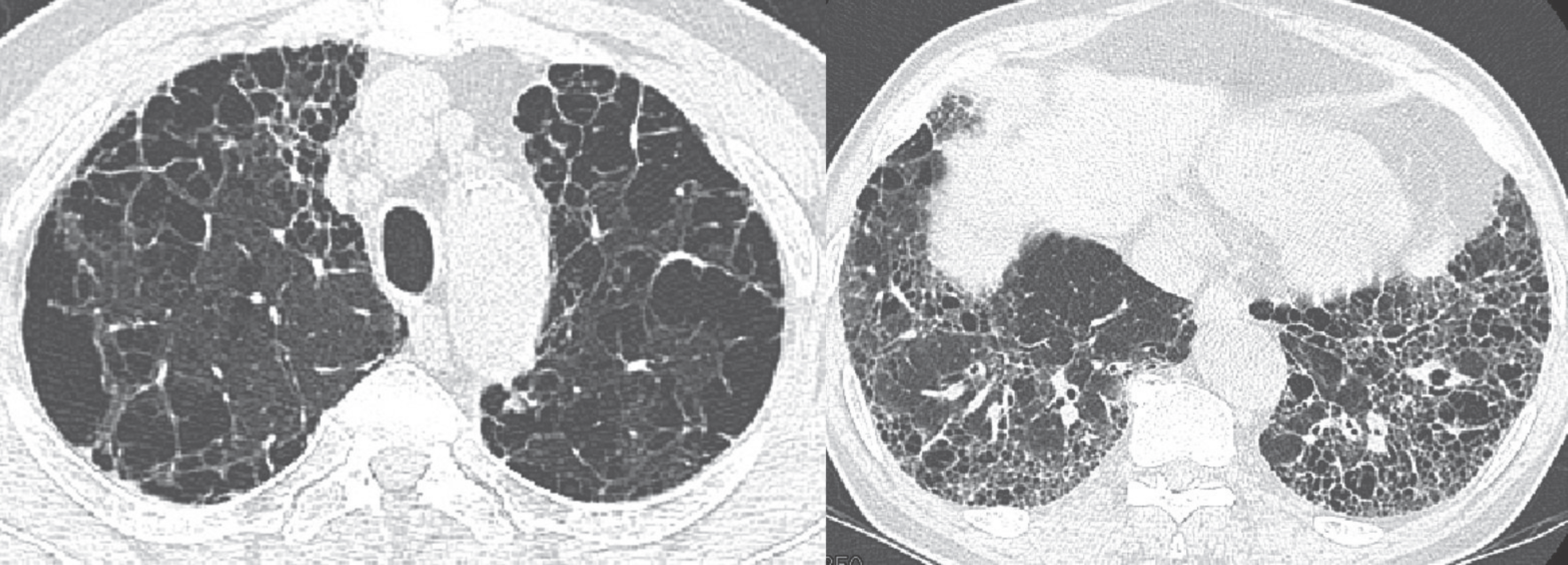
Fig. 13 Combined pulmonary fibrosis and emphysema in a 71-year-old man. Axial image of upper lungs shows emphysema, and axial CT image of lower lungs shows honeycombing appearance suggesting usual interstitial pneumonia.
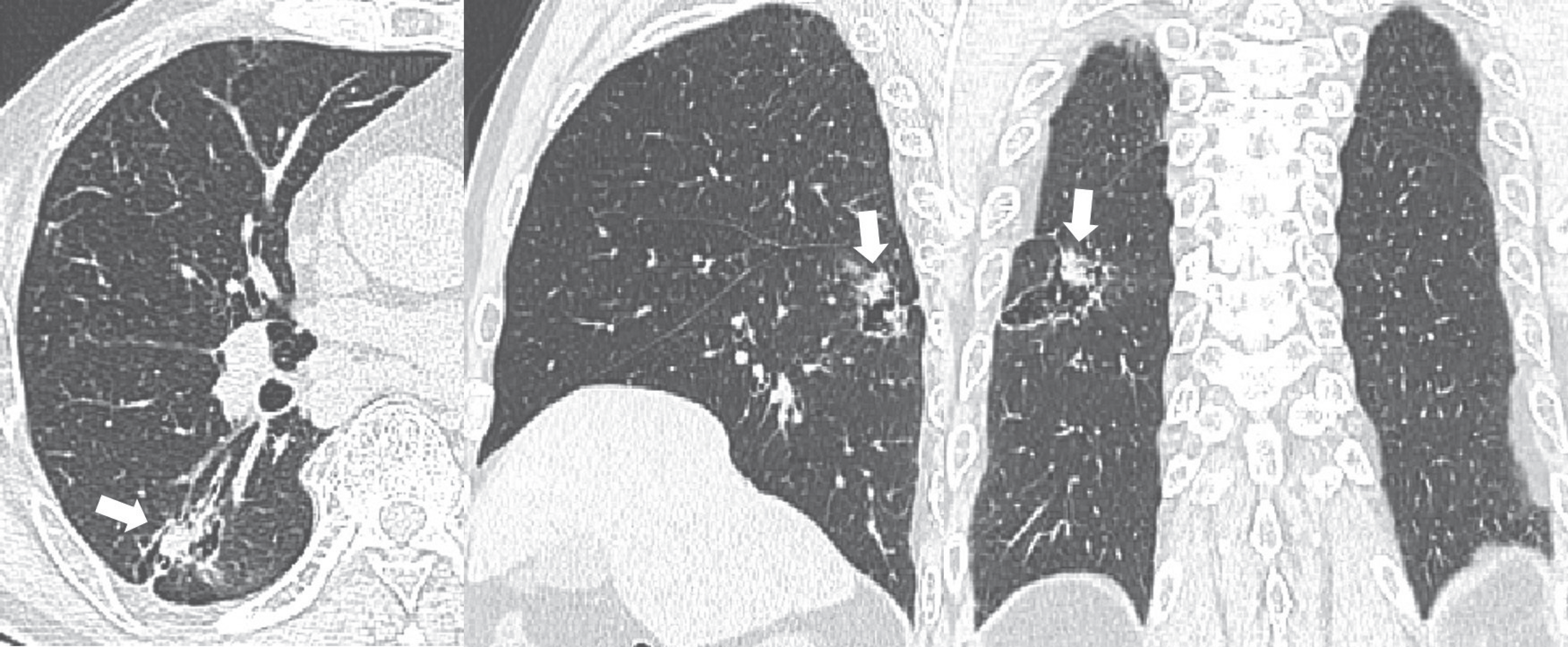
Fig. 14 Lung cancer developing in a bulla in a 79-year-old man. CT images show an irregular-shaped nodule (arrows) in a bulla in the right lower lobe. This nodule was confirmed as moderately differentiated squamous cell carcinoma by percutaneous transthoracic needle biopsy.
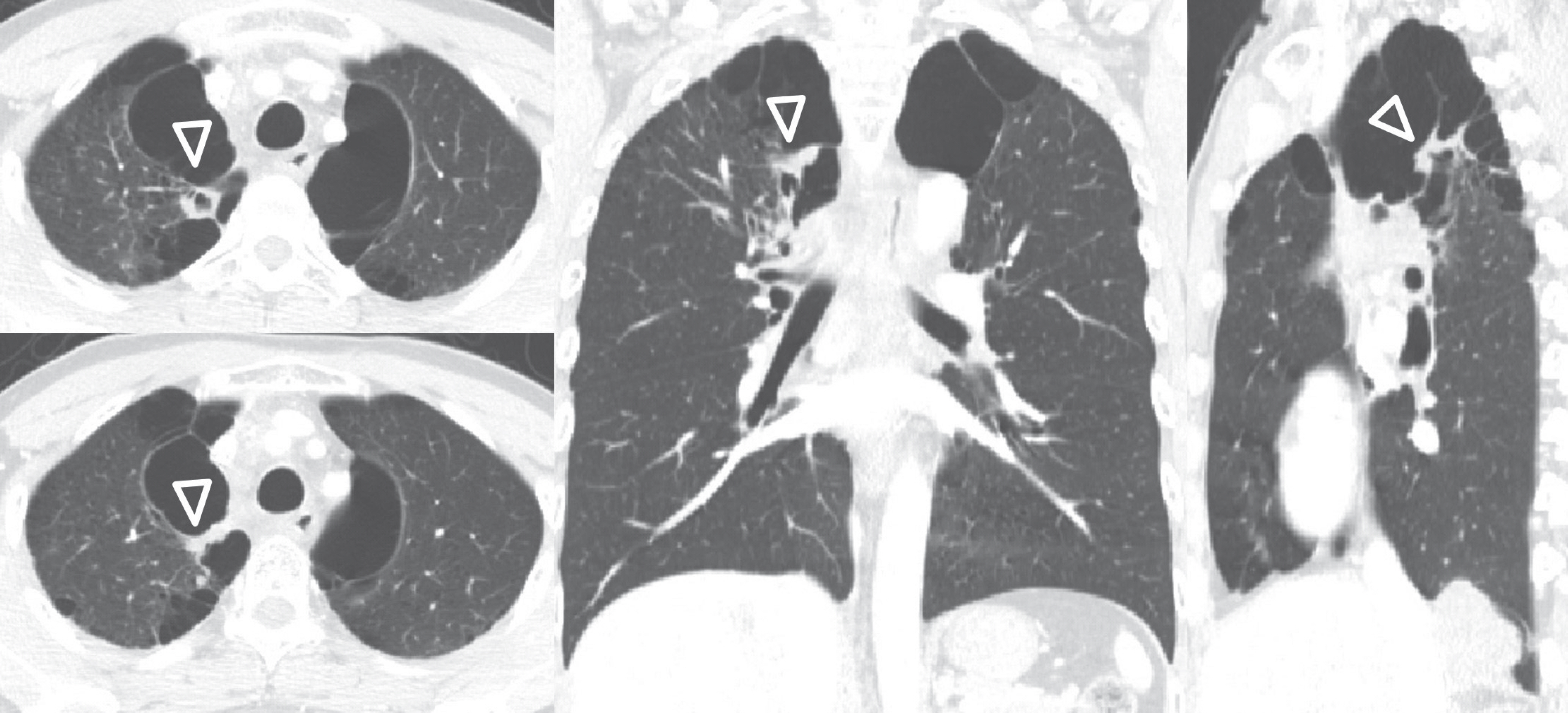
Fig. 15 Lung cancer developing in a bulla in a 79-year-old man. CT images show irregular wall thickening (arrowheads) in a bulla in the right upper lobe. This wall thickening was confirmed as poorly differentiated squamous cell carcinoma by percutaneous transthoracic needle biopsy.

Fig. 16 Spontaneous pulmonary hematoma and hemorrhage in a 54-year-old man. A. Initial CT image shows small bullae (arrow) in the right upper lobe. B. Follow-up CT images show a high-attenuation hematoma (arrow) in the bullae. Pulmonary hemorrhage (arrowheads) is also noted in the adjacent lung.

Fig. 17 Spontaneous pulmonary hematoma and hemorrhage in a 46-year-old man. A. Initial CT images show high-attenuation consolidation and diffuse ground glass opacities with Swiss cheese-like appearance in the left upper lobe. B. On sequential CT images, high-attenuation consolidation in the left upper lobe has decreased.
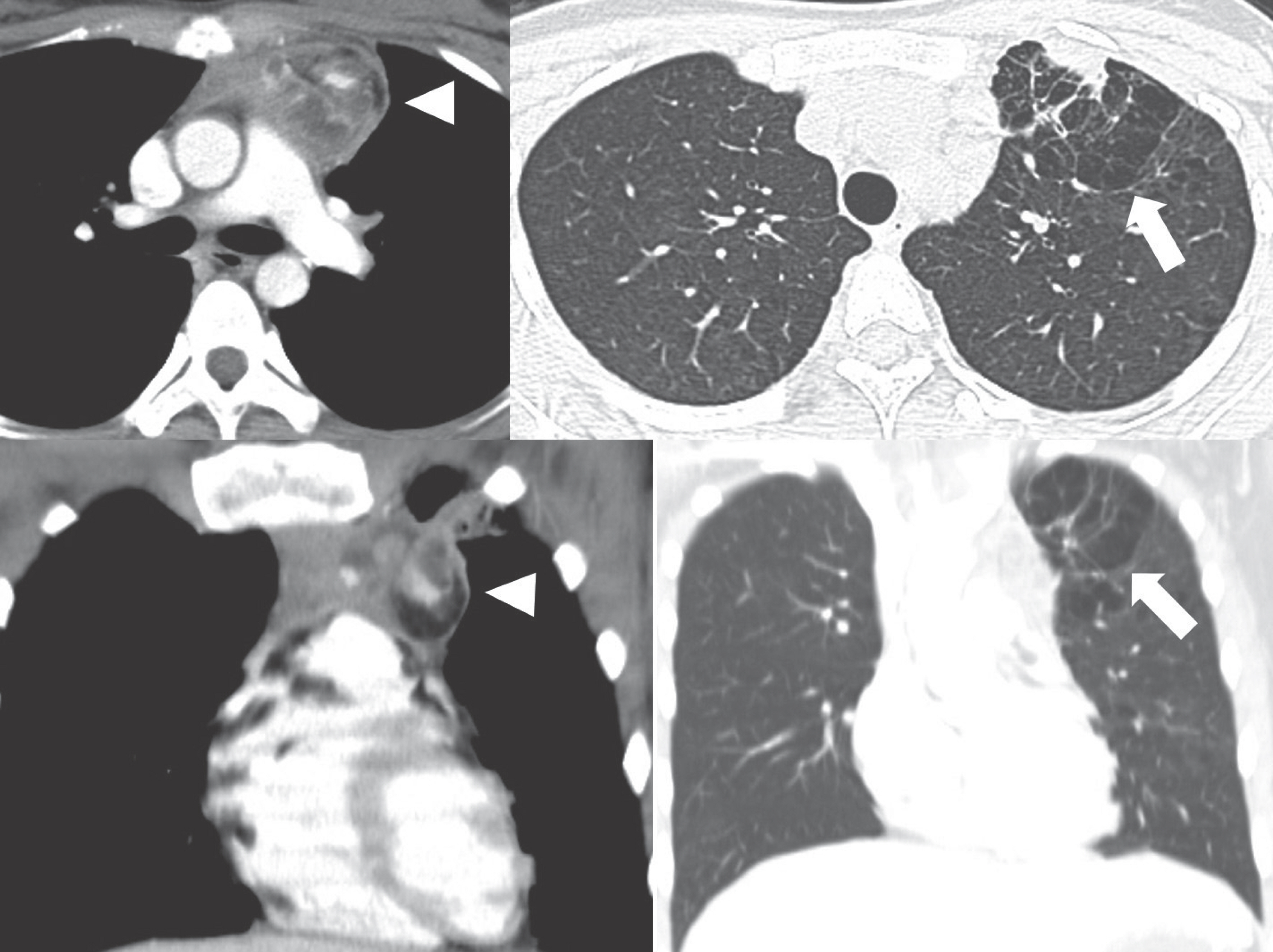
Fig. 18 Combined emphysema with mediastinal dermoid cyst in a 21-year-old woman. CT images show a mediastinal dermoid cyst (arrowheads) containing fat and calcification in the left anterior mediastinum and focal emphysema (arrows) in the adjacent left upper lobe.
Reference
-
1.Chatila WM., Thomashow BM., Minai OA., Criner GJ., Make BJ. Comorbidities in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2008. 5:549–555.
Article2.Cavaillès A., Brinchault-Rabin G., Dixmier A., Goupil F., Gut-Gobert C., Marchand-Adam S, et al. Comorbidities of COPD. Eur Respir Rev. 2013. 22:454–475.3.Cleverley JR., Müller NL. Advances in radiologic assessment of chronic obstructive pulmonary disease. Clin Chest Med. 2000. 21:653–663.
Article4.Friedman PJ. Imaging studies in emphysema. Proc Am Thorac Soc. 2008. 5:494–500.
Article5.Takasugi JE., Godwin JD. Radiology of chronic obstructive pulmonary disease. Radiol Clin North Am. 1998. 36:29–55.
Article6.Sethi S. Infection as a comorbidity of COPD. Eur Respir J. 2010. 35:1209–1215.
Article7.Juhl KS., Bendstrup E., Rasmussen F., Hilberg O. Emphysema mimicking interstitial lung disease: two case reports. Respir Med Case Rep. 2015. 15:24–26.
Article8.Nambu A., Ozawa K., Kobayashi N., Tago M. Imaging of community-acquired pneumonia: roles of imaging examinations, imaging diagnosis of specific pathogens and discrimination from noninfectious diseases. World J Radiol. 2014. 6:779–793.
Article9.Ziskind MM., Schwarz MI., George RB., Weill H., Shames JM., Herbert SJ, et al. Incomplete consolidation in pneumococcal lobar pneumonia complicating pulmonary emphysema. Ann Intern Med. 1970. 72:835–839.
Article10.Chandra D., Rose SR., Carter RB., Musher DM., Hamill RJ. Fluid-containing emphysematous bullae: a spectrum of illness. Eur Respir J. 2008. 32:303–306.
Article11.Kim YT., Han KS., Kim YI. [Parenchymal air-fluid level in emphysematous lung: a report of two cases]. J Korean Radiol Soc. 1999. 40:713–715.12.Morgan MD., Edwards CW., Morris J., Matthews HR. Origin and behaviour of emphysematous bullae. Thorax. 1989. 44:533–538.
Article13.Boushy SF., Kohen R., Billig DM., Heiman MJ. Bullous emphysema: clinical, roentgenologic and physiologic study of 49 patients. Dis Chest. 1968. 54:327–334.
Article14.Bradshaw DA., Murray KM., Amundson DE. Spontaneous regression of a giant pulmonary bulla. Thorax. 1996. 51:549–550.
Article15.Byrd RP Jr., Roy TM. Spontaneous partial resolution of a giant pulmonary bulla. Austin J Pulm Respir Med. 2014. 1:1017–1020.16.Bonay M., Debray MP. Rapid improvement in pulmonary function after inflammatory autobullectomy. Eur J Intern Med. 2008. 19:e99–e100.
Article17.Worthy SA., Brown MJ., Müller NL. Technical report: cystic air spaces in the lung: change in size on expiratory high-resolution CT in 23 patients. Clin Radiol. 1998. 53:515–519.
Article18.Nakajima J., Takamoto S., Tanaka M., Takeuchi E., Murakawa T. Thoracoscopic resection of the pulmonary aspergilloma: report of two cases. Chest. 2000. 118:1490–1492.19.Katzenstein AL., Mukhopadhyay S., Zanardi C., Dexter E. Clinically occult interstitial fibrosis in smokers: classification and significance of a surprisingly common finding in lobectomy specimens. Hum Pathol. 2010. 41:316–325.
Article20.Wright JL., Tazelaar HD., Churg A. Fibrosis with emphysema. Histopathology. 2011. 58:517–524.
Article21.Hiwatari N., Shimura S., Takishima T. Pulmonary emphysema followed by pulmonary fibrosis of undetermined cause. Respiration. 1993. 60:354–358.
Article22.Fujita J., Sato K., Irino S. Emphysematous modification of diffuse centrilobular lesions due to staphylococcal pneumonia. AJR Am J Roentgenol. 1991. 156:1322–1323.
Article23.Papiris SA., Triantafillidou C., Manali ED., Kolilekas L., Baou K., Kagouridis K, et al. Combined pulmonary fibrosis and emphysema. Expert Rev Respir Med. 2013. 7:19–31. quiz 32.
Article24.Cottin V., Cordier JF. Combined pulmonary fibrosis and emphysema: an experimental and clinically relevant phenotype. Am J Respir Crit Care Med. 2005. 172:1605;author reply. 1605–1606.
Article25.Auerbach O., Garfinkel L., Hammond EC. Relation of smoking and age to findings in lung parenchyma: a microscopic study. Chest. 1974. 65:29–35.
Article26.Katzenstein AL. Smoking-related interstitial fibrosis (SRIF): pathologic findings and distinction from other chronic fibrosing lung diseases. J Clin Pathol. 2013. 66:882–887.
Article27.Kawabata Y., Hoshi E., Murai K., Ikeya T., Takahashi N., Saitou Y, et al. Smoking-related changes in the background lung of specimens resected for lung cancer: a semiquantitative study with correlation to postoperative course. Histopathology. 2008. 53:707–714.
Article28.Watanabe Y., Kawabata Y., Kanauchi T., Hoshi E., Kurashima K., Koyama S, et al. Multiple, thin-walled cysts are one of the HRCT features of airspace enlargement with fibrosis. Eur J Radiol. 2015. 84:986–992.
Article29.Goldstein MJ., Snider GL., Liberson M., Poske RM. Bronchogenic carcinoma and giant bullous disease. Am Rev Respir Dis. 1968. 97:1062–1070.30.Hanaoka N., Tanaka F., Otake Y., Yanagihara K., Nakagawa T., Kawano Y, et al. Primary lung carcinoma arising from emphysematous bullae. Lung Cancer. 2002. 38:185–191.
Article31.Stoloff IL., Kanofsky P., Magilner L. The risk of lung cancer in males with bullous disease of the lung. Arch Environ Health. 1971. 22:163–167.
Article32.Farooqi AO., Cham M., Zhang L., Beasley MB., Austin JH., Miller A, et al. Lung cancer associated with cystic airspaces. AJR Am J Roentgenol. 2012. 199:781–786.
Article33.Ogawa D., Shiota Y., Marukawa M., Hiyama J., Mashiba H., Yu-noki K, et al. Lung cancer associated with pulmonary bulla. case report and review of literature. Respiration. 1999. 66:555–558.34.Maki D., Takahashi M., Murata K., Sawai S., Fujino S., Inoue S. Computed tomography appearances of bronchogenic carcinoma associated with bullous lung disease. J Comput Assist Tomogr. 2006. 30:447–452.
Article35.Withey S., Tamimi A. Spontaneous pulmonary haemorrhage into an existing emphysematous bulla. BMJ Case Rep. 2016. 2016:bcr2015213144.
Article36.Lee EJ., Park SH., Park HH., Park SH., Lee JY., Lee WS, et al. Spontaneous pulmonary hematoma with no underlying causes: a case report. Tuberc Respir Dis (Seoul). 2015. 78:363–365.
Article37.Nakamura S., Kawaguchi K., Fukui T., Fukumoto K., Okasaka T., Yokoi K. The development of large-cell carcinoma in the wall of a giant bulla complicated by hemorrhage. Surg Case Rep. 2016. 2:22.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical use of chest CT in chronic obstructive pulmonary diseases
- Pulmonary Emphysema: Visual Interpretation and Quantitative Analysis
- Clinical Characteristics of Chronic Obstructive Pulmonary Disease according to Smoking Status
- The Single Lung Transplantation for End-Stage Emphysema by Functional Criteria
- A Case of Pulmonary Sequestration and Congenital Lobar Emphysema Presenting with Congestive Heart Failure and Pulmonary Hypertension
