J Gastric Cancer.
2018 Mar;18(1):90-98. 10.5230/jgc.2018.18.e10.
Successful Robotic Gastrectomy Does Not Require Extensive Laparoscopic Experience
- Affiliations
-
- 1Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. jmoon.bae@samsung.com
- 2Statistics and Data Center, Research Institute for Future Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Mathematics, Ajou University, Suwon, Korea.
- KMID: 2414550
- DOI: http://doi.org/10.5230/jgc.2018.18.e10
Abstract
- PURPOSE
We evaluated the learning curve and short-term surgical outcomes of robot-assisted distal gastrectomy (RADG) performed by a single surgeon experienced in open, but not laparoscopic, gastrectomy. We aimed to verify the feasibility of performing RADG without extensive laparoscopic experience.
MATERIALS AND METHODS
Between July 2012 and December 2016, 60 RADG procedures were performed by a single surgeon using the da Vinci® Surgical System (Intuitive Surgical). Patient characteristics, the length of the learning curve, surgical parameters, and short-term postoperative outcomes were analyzed and compared before and after the learning curve had been overcome.
RESULTS
The duration of surgery rapidly decreased from the first to the fourth case; after 25 procedures, the duration of surgery was stabilized, suggesting that the learning curve had been overcome. Cases were divided into 2 groups: 25 cases before the learning curve had been overcome (early cases) and 35 later cases. The mean duration of surgery was 420.8 minutes for the initial cases and 281.7 minutes for the later cases (P<0.001). The console time was significantly shorter during the later cases (168.6 minutes) than during the early cases (247.1 minutes) (P<0.001). Although the volume of blood loss during surgery declined over time, there was no significant difference between the early and later cases. No other postoperative outcomes differed between the 2 groups. Pathology reports revealed the presence of mucosal invasion in 58 patients and submucosal invasion in 2 patients.
CONCLUSIONS
RADG can be performed safely with acceptable surgical outcomes by experts in open gastrectomy.
Figure
-
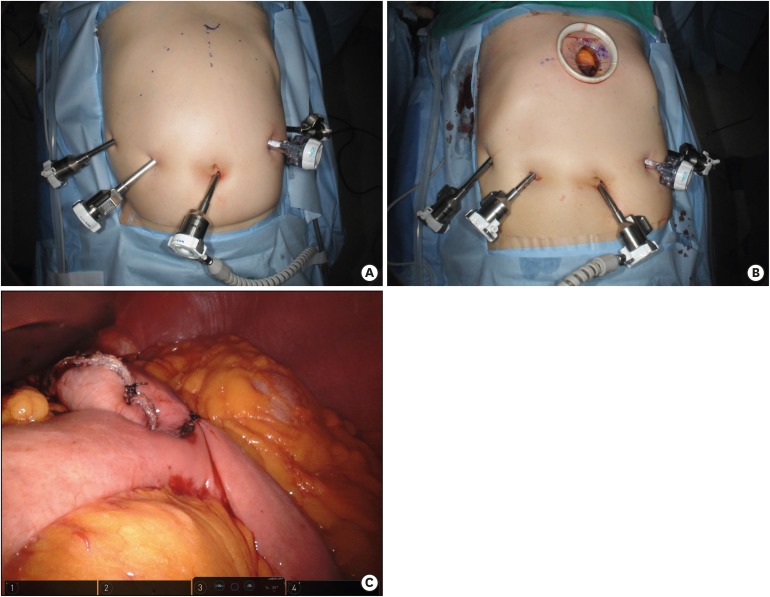
Fig. 1 Operative procedures of robot-assisted distal gastrectomy. (A) Port placements. (B) Mini-laparotomy for gastric resection and anastomosis. (C) Completion of distal gastrectomy and gastrojejunostomy.
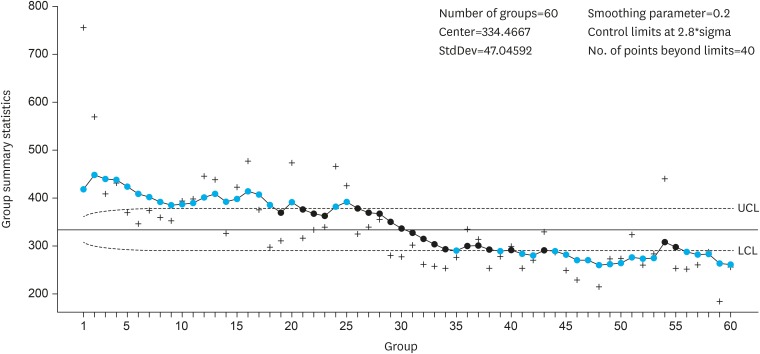
Fig. 2 Learning curve analysis using the EWMA method.EWMA = exponential weighted moving average; UCL = upper control limit; LCL = lower control limit.The learning curve was overcome after 25 cases.
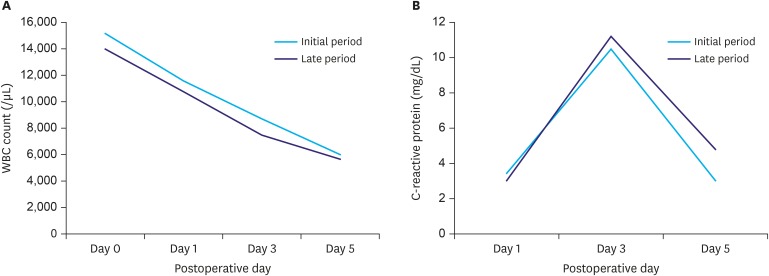
Fig. 3 Postoperative inflammation. (A) WBC counts; (B) CRP levels.WBC = white blood cell; CRP = C- reactive protein; POD = postoperative day.
Reference
-
1. Palep JH. Robotic assisted minimally invasive surgery. J Minim Access Surg. 2009; 5:1–7. PMID: 19547687.
Article2. Wexner SD, Bergamaschi R, Lacy A, Udo J, Brolmann H, Kennedy RH, et al. The current status of robotic pelvic surgery: results of a multinational interdisciplinary consensus conference. Surg Endosc. 2009; 23:438–443. PMID: 19037694.
Article3. Antoniou SA, Antoniou GA, Koch OO, Pointner R, Granderath FA. Robot-assisted laparoscopic surgery of the colon and rectum. Surg Endosc. 2012; 26:1–11. PMID: 21858568.
Article4. Patel VR, Thaly R, Shah K. Robotic radical prostatectomy: outcomes of 500 cases. BJU Int. 2007; 99:1109–1112. PMID: 17437441.
Article5. Ruiter JG, Bonnema GM, van der Voort MC, Broeders IA. Robotic control of a traditional flexible endoscope for therapy. J Robot Surg. 2013; 7:227–234. PMID: 27000918.
Article6. Jung KW, Won YJ, Oh CM, Kong HJ, Lee DH, Lee KH, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2014. Cancer Res Treat. 2017; 49:292–305. PMID: 28279062.
Article7. Information Committee of Korean Gastric Cancer Association. Korean Gastric Cancer Association nationwide survey on gastric cancer in 2014. J Gastric Cancer. 2016; 16:131–140. PMID: 27752390.8. Hong SS, Son SY, Shin HJ, Cui LH, Hur H, Han SU. Can robotic gastrectomy surpass laparoscopic gastrectomy by acquiring long-term experience? A propensity score analysis of a 7-year experience at a single institution. J Gastric Cancer. 2016; 16:240–246. PMID: 28053810.
Article9. Kim YW, Reim D, Park JY, Eom BW, Kook MC, Ryu KW, et al. Role of robot-assisted distal gastrectomy compared to laparoscopy-assisted distal gastrectomy in suprapancreatic nodal dissection for gastric cancer. Surg Endosc. 2016; 30:1547–1552. PMID: 26169636.
Article10. Park SS, Kim MC, Park MS, Hyung WJ. Rapid adaptation of robotic gastrectomy for gastric cancer by experienced laparoscopic surgeons. Surg Endosc. 2012; 26:60–67. PMID: 21789643.
Article11. Cianchi F, Indennitate G, Trallori G, Ortolani M, Paoli B, Macri G, et al. Robotic vs laparoscopic distal gastrectomy with D2 lymphadenectomy for gastric cancer: a retrospective comparative mono-institutional study. BMC Surg. 2016; 16:65. PMID: 27646414.
Article12. Kosanovic R, Romero RJ, Donkor C, Sarasua A, Rabaza JR, Gonzalez AM. A comparative retrospective study of robotic sleeve gastrectomy vs robotic gastric bypass. Int J Med Robot. 2015; 11:275–283.
Article13. Kim HI, Han SU, Yang HK, Kim YW, Lee HJ, Ryu KW, et al. Multicenter prospective comparative study of robotic versus laparoscopic gastrectomy for gastric adenocarcinoma. Ann Surg. 2016; 263:103–109. PMID: 26020107.
Article14. Marano A, Choi YY, Hyung WJ, Kim YM, Kim J, Noh SH. Robotic versus laparoscopic versus open gastrectomy: a meta-analysis. J Gastric Cancer. 2013; 13:136–148. PMID: 24156033.
Article15. Wang Z, Wang Y, Liu Y. Comparison of short outcomes between laparoscopic and experienced robotic gastrectomy: a meta-analysis and systematic review. J Minim Access Surg. 2017; 13:1–6. PMID: 27251844.16. Shen WS, Xi HQ, Chen L, Wei B. A meta-analysis of robotic versus laparoscopic gastrectomy for gastric cancer. Surg Endosc. 2014; 28:2795–2802. PMID: 24789136.
Article17. Liao G, Chen J, Ren C, Li R, Du S, Xie G, et al. Robotic versus open gastrectomy for gastric cancer: a meta-analysis. PLoS One. 2013; 8:e81946. PMID: 24312610.
Article18. Roberts SW. Control chart tests based on geometric moving averages. Technometrics. 1959; 1:239–250.
Article19. Montgomery DC. Introduction to Statistical Quality Control. 5th ed. New York (NY): John Wiley & Sons;2005.20. Lucas JM, Saccucci MS. Exponentially weighted moving average control schemes: properties and enhancements. Technometrics. 1990; 32:1–12.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Current status of robotic gastrectomy for gastric cancer: A review of recent randomized controlled trials
- Robotic Gastrectomy for Gastric Cancer: A Review of Postoperative and Oncologic Outcomes
- Robotic Roux-en-Y Gastric Bypass and Robotic Sleeve Gastrectomy for Morbid Obesity: Case Reports
- Comparison of Surgical Skills in Laparoscopic and Robotic Tasks Between Experienced Surgeons and Novices in Laparoscopic Surgery: An Experimental Study
- Robotic Surgery for Early Gastric Cancer
