Novel Endoscopic Stent for Anastomotic Leaks after Total Gastrectomy Using an Anchoring Thread and Fully Covering Thick Membrane: Prevention of Embedding and Migration
- Affiliations
-
- 1Department of Internal Medicine, Presbyterian Medical Center, Jeonju, Korea.
- 2Department of Internal Medicine, Chonnam National University Medical School, Gwangju, Korea. portalvein@naver.com
- 3Department of Surgery, Chonnam National University Medical School, Gwangju, Korea.
- KMID: 2414545
- DOI: http://doi.org/10.5230/jgc.2018.18.e2
Abstract
- PURPOSE
The endoscopic management of a fully covered self-expandable metal stent (SEMS) has been suggested for the primary treatment of patients with anastomotic leaks after total gastrectomy. Embedded stents due to tissue ingrowth and migration are the main obstacles in endoscopic stent management.
MATERIALS AND METHODS
The effectiveness and safety of endoscopic management were evaluated for anastomotic leaks when using a benign fully covered SEMS with an anchoring thread and thick silicone covering the membrane to prevent stent embedding and migration. We retrospectively reviewed the data of 14 consecutive patients with gastric cancer and anastomotic leaks after total gastrectomy treated from January 2009 to December 2016.
RESULTS
The technical success rate of endoscopic stent replacement was 100%, and the rate of complete leaks closure was 85.7% (n=12). The mean size of leaks was 13.1 mm (range, 3-30 mm). The time interval from operation to stent replacement was 10.7 days (range, 3-35 days) and the interval from stent replacement to extraction was 32.3 days (range, 18-49 days). The complication rate was 14.1%, and included a single jejunal ulcer and delayed stricture at the site of leakage. No embedded stent or migration occurred. Two patients died due to progression of pneumonia and septic shock 2 weeks after stent replacement.
CONCLUSIONS
A benign fully covered SEMS with an anchoring thread and thick membrane is an effective and safe stent in patients with anastomotic leaks after total gastrectomy. The novelty of this stent is that it provides complete prevention of stent migration and embedding, compared with conventional fully covered SEMS.
MeSH Terms
Figure
-
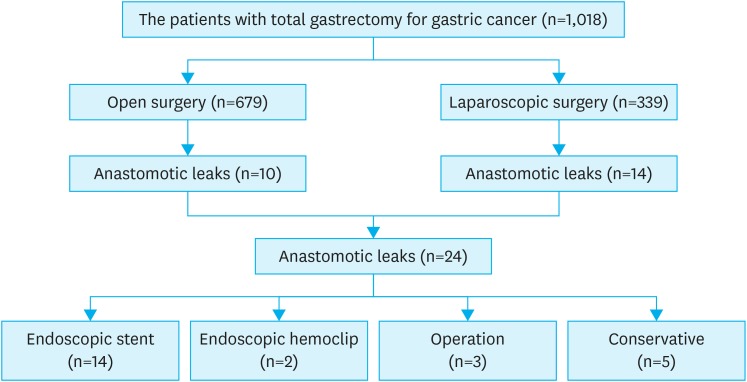
Fig. 1 The flow chart of patients with anastomotic leaks after total gastrectomy for gastric cancer.
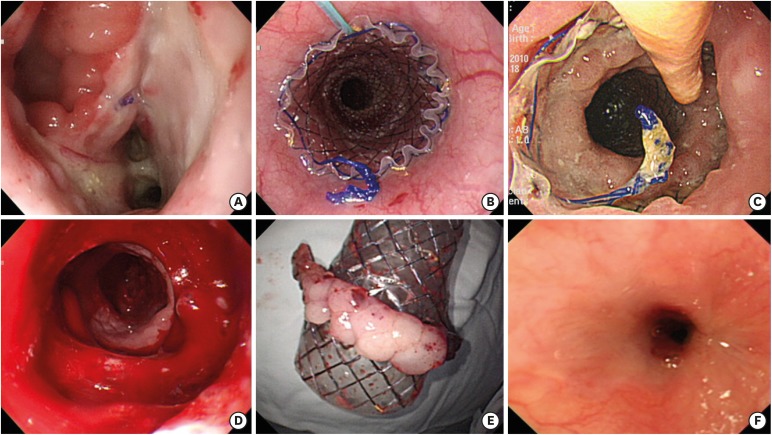
Fig. 2 Embedded stent was a major complication after the use of a conventional fully SEMS in a patient with leaks. (A) Large dehiscence at esophagojejunal anastomosis site after total gastrectomy. (B) Endoscopic placement of conventional fully SEMS. (C) Severe circumferential embedded stent after 4 weeks. (D) The stent was removed with difficulty under endoscopic and fluoroscopic guide. (E) Removed stent with attaching hyperplastic mucosa at compressed area. (F) Delayed severe stricture developed at mid esophagus with refractoriness to repeated endoscopic balloon dilatation. The patient finally underwent a second operation after 1 year.SEMS, self-expandable metal stent.

Fig. 3 Placement of a benign fully covered SEMS with thick membrane and Shim's technique. (A) Large dehiscence at esophagojejunal anastomosis site (B) fully SEMS with thick and long membrane (white arrow) and silk thread (yellow arrow). (C) No leakage after infusion of gastrografin under fluoroscopy. (D) No embedded stent without any tissue hyperplasia after 4 weeks. (E) Near complete sealing of dehiscence in prechecking endoscopy before removal after 4 weeks. (F) The removal of the stent was delayed to 1 week, and the leaks were completely sealed after 5 weeks.SEMS, self-expandable metal stent.

Fig. 4 An additional feeding tube was inserted into the deep jejunum below the stent under endoscopic and fluoroscopic guide (A). This is helpful to improve nutritional status and to decrease food leakage through the space of esophageal wall and stent (B).
Reference
-
1. Griffin SM, Lamb PJ, Dresner SM, Richardson DL, Hayes N. Diagnosis and management of a mediastinal leak following radical oesophagectomy. Br J Surg. 2001; 88:1346–1351. PMID: 11578290.
Article2. Pross M, Manger T, Reinheckel T, Mirow L, Kunz D, Lippert H. Endoscopic treatment of clinically symptomatic leaks of thoracic esophageal anastomoses. Gastrointest Endosc. 2000; 51:73–76. PMID: 10625803.
Article3. Alanezi K, Urschel JD. Mortality secondary to esophageal anastomotic leak. Ann Thorac Cardiovasc Surg. 2004; 10:71–75. PMID: 15209546.4. DaVee T, Irani S, Leggett CL, Berzosa Corella M, Grooteman KV, Wong Kee Song LM, et al. Stent-in-stent technique for removal of embedded partially covered self-expanding metal stents. Surg Endosc. 2016; 30:2332–2341. PMID: 26416379.
Article5. Langer FB, Schoppmann SF, Prager G, Riegler FM, Zacherl J. Solving the problem of difficult stent removal due to tissue ingrowth in partially uncovered esophageal self-expanding metal stents. Ann Thorac Surg. 2010; 89:1691–1692. PMID: 20417822.
Article6. Shim CS, Cho YD, Moon JH, Kim JO, Cho JY, Kim YS, et al. Fixation of a modified covered esophageal stent: its clinical usefulness for preventing stent migration. Endoscopy. 2001; 33:843–848. PMID: 11571679.
Article7. Rutegård M, Lagergren P, Rouvelas I, Lagergren J. Intrathoracic anastomotic leakage and mortality after esophageal cancer resection: a population-based study. Ann Surg Oncol. 2012; 19:99–103. PMID: 21769467.
Article8. Swinnen J, Eisendrath P, Rigaux J, Kahegeshe L, Lemmers A, Le Moine O, et al. Self-expandable metal stents for the treatment of benign upper GI leaks and perforations. Gastrointest Endosc. 2011; 73:890–899. PMID: 21521563.
Article9. Suzuki T, Siddiqui A, Taylor LJ, Cox K, Hasan RA, Laique SN, et al. Clinical outcomes, efficacy, and adverse events in patients undergoing esophageal stent placement for benign indications: a large multicenter study. J Clin Gastroenterol. 2016; 50:373–378. PMID: 26905604.10. Shim CN, Kim HI, Hyung WJ, Noh SH, Song MK, Kang DR, et al. Self-expanding metal stents or nonstent endoscopic therapy: which is better for anastomotic leaks after total gastrectomy? Surg Endosc. 2014; 28:833–840. PMID: 24114516.
Article11. Choi CW, Kang DH, Kim HW, Park SB, Kim SJ, Hwang SH, et al. Full covered self-expandable metal stents for the treatment of anastomotic leak using a silk thread. Medicine (Baltimore). 2017; 96:e7439. PMID: 28723752.
Article12. van Boeckel PG, Sijbring A, Vleggaar FP, Siersema PD. Systematic review: temporary stent placement for benign rupture or anastomotic leak of the oesophagus. Aliment Pharmacol Ther. 2011; 33:1292–1301. PMID: 21517921.
Article13. Salminen P, Gullichsen R, Laine S. Use of self-expandable metal stents for the treatment of esophageal perforations and anastomotic leaks. Surg Endosc. 2009; 23:1526–1530. PMID: 19301070.
Article14. van Halsema EE, Wong Kee Song LM, Baron TH, Siersema PD, Vleggaar FP, Ginsberg GG, et al. Safety of endoscopic removal of self-expandable stents after treatment of benign esophageal diseases. Gastrointest Endosc. 2013; 77:18–28. PMID: 23261092.
Article15. Wadhwa RP, Kozarek RA, France RE, Brandabur JJ, Gluck M, Low DE, et al. Use of self-expandable metallic stents in benign GI diseases. Gastrointest Endosc. 2003; 58:207–212. PMID: 12872087.
Article16. Chaput U, Heresbach D, Audureau E, Vanbiervliet G, Gaudric M, Bichard P, et al. Comparison of a standard fully covered stent with a super-thick silicone-covered stent for the treatment of refractory esophageal benign strictures: a prospective multicenter study. United European Gastroenterol J. 2013; 1:93–102.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Enteral stents in the management of gastrointestinal leaks, perforations and fistulae
- A Case of Endoscopic Stenting for Anastomotic Leakage after Total Gastrectomy
- Plastic and Biodegradable Stents for Complex and Refractory Benign Esophageal Strictures
- Endoscopic Intervention for Anastomotic Leakage After Gastrectomy
- Role of Fully Covered Self-Expandable Metal Stent for Treatment of Benign Biliary Strictures and Bile Leaks
