Cost-Effectiveness Estimate for Neural Monitoring in Thyroid Surgery
- Kim HY

- Chai YJ
- Freni F
- Makay O
- Galletti B
- Galletti F
- Sun H
- Dionigi G
- The Korean Intraoperative Neural Monitoring Society (KINMoS)
- Affiliations
-
- 1KUMC Thyroid Center, Korea University Anam Hospital, Seoul, Korea.
- 2Department of Surgery, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul, Korea.
- 3Division for ENT Surgery, Department of Human Pathology in Adulthood and Childhood “G. Barresiâ€, University Hospital G. Martino, University of Messina, Messina, Italy.
- 4Division of Endocrine Surgery, Department of General Surgery, Ege University Hospital, Izmir, Turkey.
- 5Division of Thyroid Surgery, Jilin Provincial Key Laboratory of Surgical Translational Medicine, China-Japan Union Hospital of Jilin University, Changchun, China.
- 6Division for Endocrine and Minimally Invasive Surgery, Department of Human Pathology in Adulthood and Childhood “G. Barresiâ€, University Hospital G. Martino, University of Messina, Messina, Italy. gdionigi@unime.it
- KMID: 2414419
- DOI: http://doi.org/10.16956/jes.2018.18.1.10
Abstract
- There is growing evidence for the importance of more detailed cost evaluation of new technologies used in surgery. The innovative impact of technology holds the potential to achieve transformative clinical improvements. Sustainability of innovations is a relatively new concept in health care research and has become an issue of growing interest. Cost-effectiveness studies have been the most established and studied methods for evaluation in surgical patients. Limited information exists regarding the cost-effectiveness of new surgical strategies for monitored thyroid surgeries. We describe the recent evidence regarding methods of evaluation of cost-effectiveness structures and function for intraoperative neural monitoring (IONM) in thyroid surgery. Our findings suggest that health economics modeling to inform the design of a cost-effectiveness studies looking at IONM has been demonstrated to be feasible as a method for improving research efficiency.
Figure
-
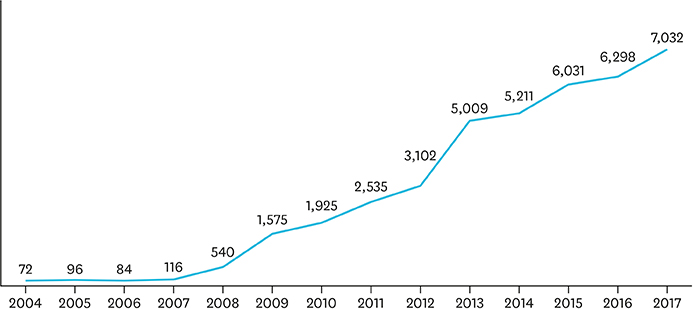
Fig. 1 Prevalence of IONM in Italy. Data from Italian consumption of electromyogram tubes. About 38 to 40,000 thyroidectomies per year are performed in Italy, that is about 16% are monitored. IONM = intraoperative neural monitoring.
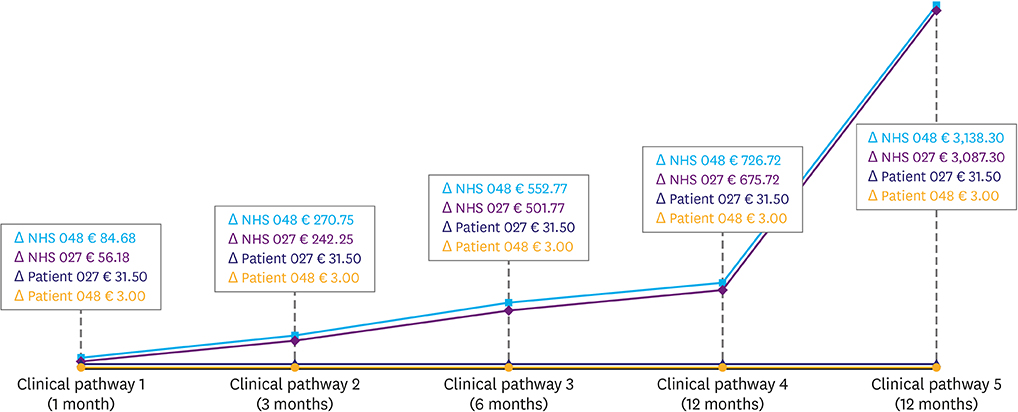
Fig. 2 Cost per RLN injury. Expense are sensitive to time-recovery (i.e., severity) of RLN injury. Figures are higher for thyroid malignant disease than benign surgery. Charges in the case of vocal cord surgery are higher than no medications. Both costs incurred by patient and NHS are significant (figure adapted from reference 27). Each clinical pathway means follow as: clinical pathway 1, RLN function recovery <1 month; clinical pathway 2, RLN function recovery ≥1 month and <3 months; clinical pathway 3, RLN function recovery ≥3 months and <6 months; clinical pathway 4, RLN function recovery ≥6 months and <12 months; clinical pathway 4, RLN function recovery ≥12 months, with phono surgery. RLN = recurrent laryngeal nerve; NHS = National Healthcare System.

Fig. 3 IONM cost-effectiveness challenges. IONM = intraoperative neural monitoring; RLNP = recurrent laryngeal nerve palsy.
Reference
-
1. Dralle H, Sekulla C, Lorenz K, Brauckhoff M, Machens A; German IONM Study Group. Intraoperative monitoring of the recurrent laryngeal nerve in thyroid surgery. World J Surg. 2008; 32:1358–1366.
Article2. Barczyński M, Konturek A, Cichoń S. Randomized clinical trial of visualization versus neuromonitoring of recurrent laryngeal nerves during thyroidectomy. Br J Surg. 2009; 96:240–246.
Article3. Horne SK, Gal TJ, Brennan JA. Prevalence and patterns of intraoperative nerve monitoring for thyroidectomy. Otolaryngol Head Neck Surg. 2007; 136:952–956.
Article4. Sturgeon C, Sturgeon T, Angelos P. Neuromonitoring in thyroid surgery: attitudes, usage patterns, and predictors of use among endocrine surgeons. World J Surg. 2009; 33:417–425.
Article5. Lamade W, Fogel W, Rieke K, Senninger N, Herfarth C. Intraoperative monitoring of the recurrent laryngeal nerve. A new method. Chirurg. 1996; 67:451–454.6. Thomusch O, Sekulla C, Walls G, Machens A, Dralle H. Intraoperative neuromonitoring of surgery for benign goiter. Am J Surg. 2002; 183:673–678.
Article7. Chiang FY, Lee KW, Chen HC, Chen HY, Lu IC, Kuo WR, et al. Standardization of intraoperative neuromonitoring of recurrent laryngeal nerve in thyroid operation. World J Surg. 2010; 34:223–229.
Article8. Randolph GW, Dralle H, Abdullah H, Barczynski M, Bellantone R, Brauckhoff M, et al. Electrophysiologic recurrent laryngeal nerve monitoring during thyroid and parathyroid surgery: international standards guideline statement. Laryngoscope. 2011; 121:Suppl 1. S1–16.
Article9. Loch-Wilkinson TJ, Stalberg PL, Sidhu SB, Sywak MS, Wilkinson JF, Delbridge LW. Nerve stimulation in thyroid surgery: is it really useful? ANZ J Surg. 2007; 77:377–380.
Article10. Frick KD. Microcosting quantity data collection methods. Med Care. 2009; 47:S76–81.
Article11. Heerey A, McGowan B, Ryan M, Barry M. Microcosting versus DRGs in the provision of cost estimates for use in pharmacoeconomic evaluation. Expert Rev Pharmacoecon Outcomes Res. 2002; 2:29–33.
Article12. Dionigi G, Bacuzzi A, Boni L, Rovera F, Dionigi R. What is the learning curve for intraoperative neuromonitoring in thyroid surgery? Int J Surg. 2008; 6:Suppl 1. S7–12.
Article13. Antos J, Elwell D. Using activity-based management to control costs & achieve organization goals. Caring. 1998; 17:34–38.14. Regione Lombardia (IT). Delibera di Giunta Regionale n. 8501 [Internet]. Milano: Regione Lombardia;2008. 11. 26. cited year month day. Available from: http://www.regione.lombardia.it.15. Sosa JA, Bowman HM, Tielsch JM, Powe NR, Gordon TA, Udelsman R. The importance of surgeon experience for clinical and economic outcomes from thyroidectomy. Ann Surg. 1998; 228:320–330.
Article16. Dionigi G, Bacuzzi A, Boni L, Rausei S, Rovera F, Dionigi R. Visualization versus neuromonitoring of recurrent laryngeal nerves during thyroidectomy: what about the costs? World J Surg. 2012; 36:748–754.
Article17. Sanguinetti A, Parmeggiani D, Lucchini R, Monacelli M, Triola R, Avenia S, et al. Intraoperative recurrent laryngeal nerve monitoring in thyroid surgery evaluation of its use in terms of “spending review”. Ann Ital Chir. 2014; 85:418–421.18. Echeverri A, Flexon PB. Electrophysiologic nerve stimulation for identifying the recurrent laryngeal nerve in thyroid surgery: review of 70 consecutive thyroid surgeries. Am Surg. 1998; 64:328–333.19. Jeannon JP, Orabi AA, Bruch GA, Abdalsalam HA, Simo R. Diagnosis of recurrent laryngeal nerve palsy after thyroidectomy: a systematic review. Int J Clin Pract. 2009; 63:624–629.
Article20. Francis DO, Randolph G, Davies L. Nationwide variation in rates of thyroidectomy among US medicare beneficiaries. JAMA Otolaryngol Head Neck Surg. 2017; 143:1122–1125.
Article21. Nouraei SA, Allen J, Kaddour H, Middleton SE, Aylin P, Darzi A, et al. Vocal palsy increases the risk of lower respiratory tract infection in low-risk, low-morbidity patients undergoing thyroidectomy for benign disease: a big data analysis. Clin Otolaryngol. 2017; 42:1259–1266.
Article22. Cohen SM, Dupont WD, Courey MS. Quality-of-life impact of non-neoplastic voice disorders: a meta-analysis. Ann Otol Rhinol Laryngol. 2006; 115:128–134.
Article23. Cohen SM, Lee HJ, Roy N, Misono S. Pharmacologic management of voice disorders by general medicine providers and otolaryngologists. Laryngoscope. Forthcoming. 2017.
Article24. Cohen SM, Kim J, Roy N, Asche C, Courey M. The impact of laryngeal disorders on work-related dysfunction. Laryngoscope. 2012; 122:1589–1594.
Article25. Cohen SM, Kim J, Roy N, Asche C, Courey M. Direct health care costs of laryngeal diseases and disorders. Laryngoscope. 2012; 122:1582–1588.
Article26. Cohen SM, Kim J, Roy N, Asche C, Courey M. Prevalence and causes of dysphonia in a large treatment-seeking population. Laryngoscope. 2012; 122:343–348.
Article27. Ferrari CC, Rausei S, Amico F, Boni L, Chiang FY, Wu CW, et al. Recurrent laryngeal nerve injury in thyroid surgery: clinical pathways and resources consumption. Head Neck. 2016; 38:1657–1665.
Article28. Cohen SM, Kim J, Roy N, Courey M. Delayed otolaryngology referral for voice disorders increases health care costs. Am J Med. 2015; 128:426.e11–426.e18.
Article29. Lang BH, Wong CK, Tsang RK, Wong KP, Wong BY. Evaluating the cost-effectiveness of laryngeal examination after elective total thyroidectomy. Ann Surg Oncol. 2014; 21:3548–3556.
Article30. Wang T, Kim HY, Wu CW, Rausei S, Sun H, Pergolizzi FP, et al. Analyzing cost-effectiveness of neural-monitoring in recurrent laryngeal nerve recovery course in thyroid surgery. Int J Surg. 2017; 48:180–188.
Article31. Sanabria Á, Ramírez A. Economic analysis of routine neuromonitoring of recurrent laryngeal nerve in total thyroidectomy. Biomedica. 2015; 35:363–371.32. Rocke DJ, Goldstein DP, de Almeida JR. A cost-utility analysis of recurrent laryngeal nerve monitoring in the setting of total thyroidectomy. JAMA Otolaryngol Head Neck Surg. 2016; 142:1199–1205.
Article33. Al-Qurayshi Z, Kandil E, Randolph GW. Cost-effectiveness of intraoperative nerve monitoring in avoidance of bilateral recurrent laryngeal nerve injury in patients undergoing total thyroidectomy. Br J Surg. 2017; 104:1523–1531.
Article34. Sun H, Wu CW, Kim HY, Dionigi G. Neural monitoring represent central safety asset for new technologies in thyroid surgery in translational protocols. Am J Surg. Forthcoming. 2018.35. Wilson L, Lin E, Lalwani A. Cost-effectiveness of intraoperative facial nerve monitoring in middle ear or mastoid surgery. Laryngoscope. 2003; 113:1736–1745.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cost-effectiveness of intraoperative neural monitoring of recurrent laryngeal nerves in thyroid lobectomy for papillary thyroid carcinoma
- A Study on the Method to Estimate the Cost of Hospice Care
- Technical Instructions for Continuous Intraoperative Neural Monitoring in Thyroid Surgery
- Intraoperative Neural Monitoring in Thyroid Surgery: Role and Responsibility of Surgeon
- Future Directions of Neural Monitoring in Thyroid Surgery
