Computational Simulation of Multiple Cannulated Screw Fixation for Femoral Neck Fractures and the Anatomic Features for Clinical Applications
- Affiliations
-
- 1Department of Orthopedic Surgery, Gyeongsang National University Changwon Hospital, Gyeongsang National University School of Medicine, Changwon, Korea. jyujin2001@hotmail.com
- KMID: 2409758
- DOI: http://doi.org/10.12671/jkfs.2018.31.2.37
Abstract
- PURPOSE
To identify the anatomic features for clinical applications through a computational simulation of the fixation of three cannulated screws for a femoral neck fracture.
MATERIALS AND METHODS
Thirty cadaveric femurs underwent computed tomography and the images were transferred to the Mimics® program, resulting in three-dimensional proximal femur models. A three-dimensional scan of the 7.0 mm cannulated screw was performed to enable computerized virtual fixation of multiple cannulated screws for femoral neck fractures. After positioning the screws definitively for cortical support, the intraosseous position of the cannulated screws was evaluated in the anteroposterior image and axial image direction.
RESULTS
Three cannulated screws located at the each ideal site showed an array of tilted triangles with anterior screw attachment and the shortest spacing between posterior and central screws. The central screw located at the lower side was placed in the mid-height of the lesser trochanter and slightly posterior, and directed toward the junction of femoral head and neck to achieve medial cortical support. All the posterior screws were limited in height by the trochanteric fossa and were located below the vastus ridge, but the anterior screws were located higher than the vastus ridge in 10 cases. To obtain the maximum spacing of the anterior and posterior screws on the axial plane, they should be positioned parallel to the cervical region nearest the cortical bone at a height not exceeding the vastus ridge.
CONCLUSION
The position of cannulated screws for cortical support were irregular triangular arrangements with the anterosuperior apex. The position of the ideal central screw in the anteroposterior view was at the mid-height of the lesser trochanter toward the junction of the femoral head and neck, and the anterior and posterior screws were parallel to the neck with a maximal spread just inferior to the vastus ridge.
Figure
-
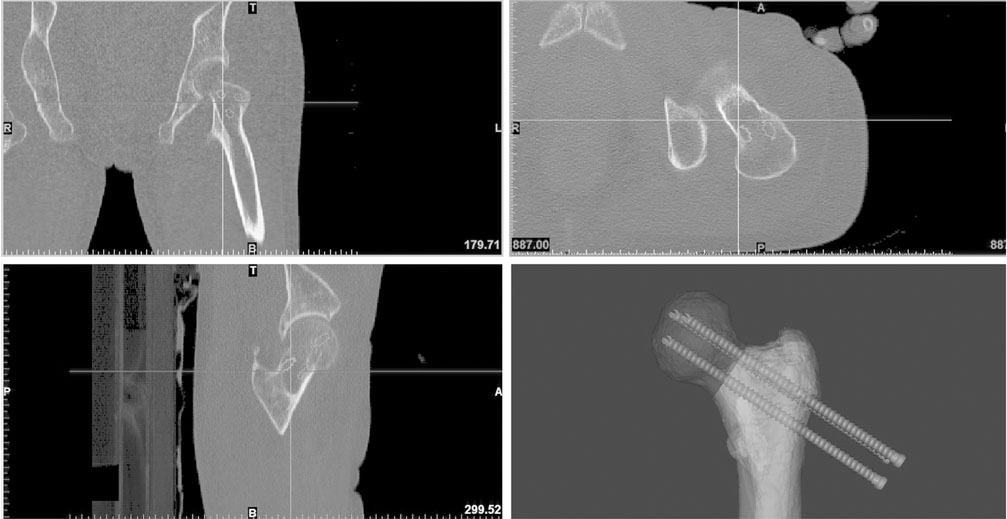
Fig. 1 Computational simulation of inserting multiple 7.0 mm cannulated screw fixation was performed using the Mimics® software, in which four synchronized windows were available.
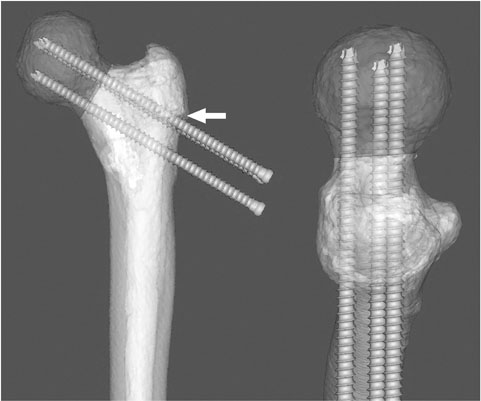
Fig. 2 After positioning the screws definitively for cortical support, the intraosseous position of cannulated screws was evaluated in the anteroposterior image and axial image direction (white arrow: vastus ridge).
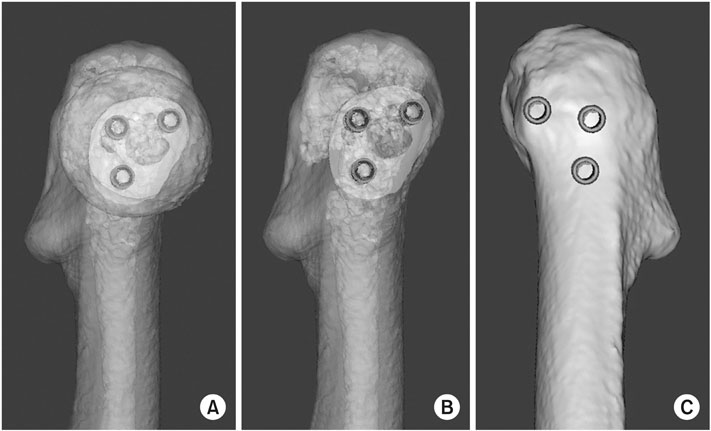
Fig. 3 (A, B) Safe zone for multiple cannulated screw fixation was clearly visible in the view of the femoral neck axis by the transparent mode. (C) The entry point of the screws was verified in the opaque mode and compared with the vastus ridge.
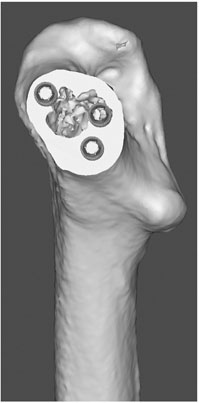
Fig. 4 Morphological features of safe zone and intraosseous position of screws were evaluated by making the cutting plane in the vertical direction of the femoral neck axis.

Fig. 5 Safe zone for cannulated screws in the femoral neck was an irregular pattern of the triangle and affected by the trochanteric fossa (*).
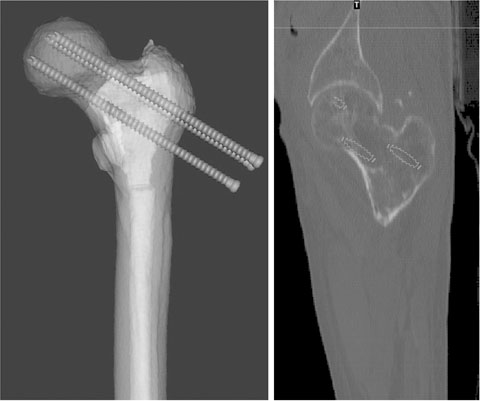
Fig. 6 Medial cortical support could be verified by the coronal image of a computational simulation but the central screw was not parallel to the femoral neck axis.

Fig. 7 Trochanteric lag screw was inserted easily between the anterior and posterior screw over the vastus ridge (white arrow).

Fig. 8 (A, B) Cortical perforation of posterosuperior quadrant occurred around the trochanteric fossa by the upward migration of the posterior screw from the ideal position. (C) In the case of cortical perforation around the trochanteric fossa, the posterior screw was located at approximately the same height as the anterior screw.
Reference
-
1. Collinge CA, Mir H, Reddix R. Fracture morphology of high shear angle “vertical” femoral neck fractures in young adult patients. J Orthop Trauma. 2014; 28:270–275.
Article2. Barquet A, Mayora G, Guimaraes JM, Suárez R, Giannoudis PV. Avascular necrosis of the femoral head following trochanteric fractures in adults: a systematic review. Injury. 2014; 45:1848–1858.
Article3. Huang TW, Hsu WH, Peng KT, Lee CY. Effect of integrity of the posterior cortex in displaced femoral neck fractures on outcome after surgical fixation in young adults. Injury. 2011; 42:217–222.
Article4. Hawks MA, Kim H, Strauss JE, et al. Does a trochanteric lag screw improve fixation of vertically oriented femoral neck fractures? A biomechanical analysis in cadaveric bone. Clin Biomech (Bristol, Avon). 2013; 28:886–891.
Article5. Hoshino CM, Christian MW, O'Toole RV, Manson TT. Fixation of displaced femoral neck fractures in young adults: fixed-angle devices or Pauwel screws? Injury. 2016; 47:1676–1684.
Article6. Ye Y, Hao J, Mauffrey C, Hammerberg EM, Stahel PF, Hak DJ. Optimizing stability in femoral neck fracture fixation. Orthopedics. 2015; 38:625–630.
Article7. Zhang YQ, Chang SM, Huang YG, Wang X. The femoral neck safe zone: a radiographic simulation study to prevent cortical perforation with multiple screw insertion. J Orthop Trauma. 2015; 29:e178–e182.8. Byun YS, Jung GH. Three-dimensional correlation between trochanteric fossa and the ideal entry point for antegrade femoral nailing. Injury. 2016; 47:2539–2543.
Article9. Gurusamy K, Parker MJ, Rowlands TK. The complications of displaced intracapsular fractures of the hip: the effect of screw positioning and angulation on fracture healing. J Bone Joint Surg Br. 2005; 87:632–634.10. Selvan VT, Oakley MJ, Rangan A, Al-Lami MK. Optimum configuration of cannulated hip screws for the fixation of intracapsular hip fractures: a biomechanical study. Injury. 2004; 35:136–141.
Article11. Grechenig W, Pichler W, Clement H, Tesch NP, Grechenig S. Anatomy of the greater femoral trochanter: clinical importance for intramedullary femoral nailing. Anatomic study of 100 cadaver specimens. Acta Orthop. 2006; 77:899–901.
Article12. Ly TV, Swiontkowski MF. Treatment of femoral neck fractures in young adults. J Bone Joint Surg Am. 2008; 90:2254–2266.13. McGrory BJ, Morrey BF, Cahalan TD, An KN, Cabanela ME. Effect of femoral offset on range of motion and abductor muscle strength after total hip arthroplasty. J Bone Joint Surg Br. 1995; 77:865–869.
Article14. Boraiah S, Paul O, Hammoud S, Gardner MJ, Helfet DL, Lorich DG. Predictable healing of femoral neck fractures treated with intraoperative compression and length-stable implants. J Trauma. 2010; 69:142–147.
Article15. Slobogean GP, Sprague SA, Scott T, McKee M, Bhandari M. Management of young femoral neck fractures: is there a consensus? Injury. 2015; 46:435–440.
Article16. Slobogean GP, Sprague SA, Scott T, Bhandari M. Complications following young femoral neck fractures. Injury. 2015; 46:484–491.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Computational Simulation of Femoral Neck System and Additional Cannulated Screws Fixation for Unstable Femoral Neck Fractures and the Biomechanical Features for Clinical Applications
- Subtrochanteric Fracture after Cannulatd Screw Fixation of Femoral Neck Fracture in a Child: A Case Report
- Treatment of Femoral Neck Fracture (Comparison of Knowles Pin and Cannulated Screw Fixation)
- Femoral Neck Fracture Fixation (Comparison of Dynamic Hip Screw and Cannulated Screw Fixation)
- Cannulated Screw Fixation for Femoral Neck Fractures
