Difference of Diagnostic Rates and Analytical Methods in the Test Positions of Vestibular Evoked Myogenic Potentials
- Affiliations
-
- 1Department of Rehabilitation Medicine, Wonju Severance Christian Hospital, Wonju, Korea. trapezium1@hanmail.net
- 2Department of Occupational Therapy, Graduate School, Yonsei University, Wonju, Korea.
- 3Department of Occupational Therapy, Wonju Medical Center, Wonju, Korea.
- 4Department of Otolaryngology-Head and Neck Surgery, Yonsei University Wonju College of Medicine, Wonju, Korea.
Abstract
OBJECTIVE
To compare the differences of diagnostic rates, of the two widely used test positions, in measuring vestibular evoked myogenic potentials (VEMP) and selecting the most appropriate analytical method for diagnostic criteria for the patients with vertigo.
METHODS
Thirty-two patients with vertigo were tested in two comparative testing positions: turning the head to the opposite side of the evaluating side and bowing while in seated position, and bowing while in supine positions. Abnormalities were determined by prolonged latency of p13 or n23, shortening of the interpeak latency, and absence of VEMP formation.
RESULTS
Using the three criteria above for determining abnormalities, both the seated and supine positions showed no significant differences in diagnostic rates, however, the concordance correlation of the two positions was low. When using only the prolonged latency of p13 or n23 in the two positions, diagnostic rates were not significantly different and their concordance correlation was high. On the other hand, using only the shortened interpeak latency in both positions showed no significant difference of diagnostic rates, and the degree of agreement between two positions was low.
CONCLUSION
Bowing while in seated position with the head turned in the opposite direction to the area being evaluated is found to be the best VEMP test position due to the consistent level of sternocleidomastoid muscle tension and the high level of compliance. Also, among other diagnostic analysis methods, using prolonged latency of p13 or n23 as the criterion is found to be the most appropriate method of analysis for the VEMP test.
MeSH Terms
Figure
-
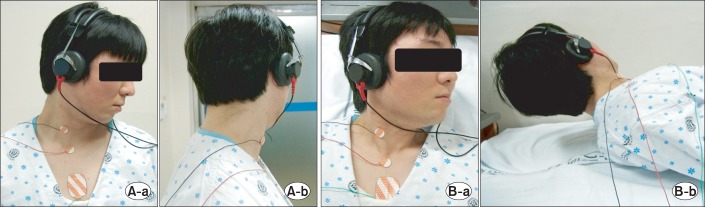
Fig. 1 Testing position. (A) Lowering one's head toward the opposite side of the testing side in seated (position 1: a, anterial; b, lateral). (B) Lifting one's head 10 cm to the opposite side of the testing side in supine (position 2: a, anterial; b, lateral).
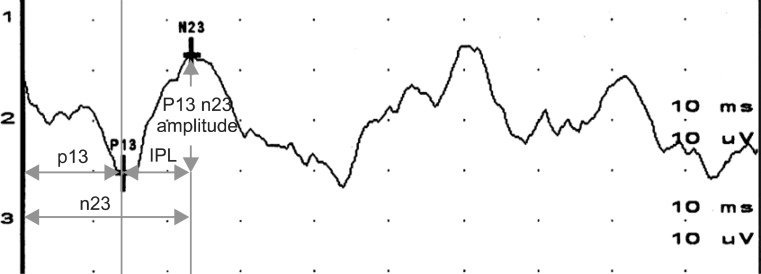
Fig. 2 Typical response and measurement parameters of vestibular evoked myogenic potentials. IPL, interpeak latency.
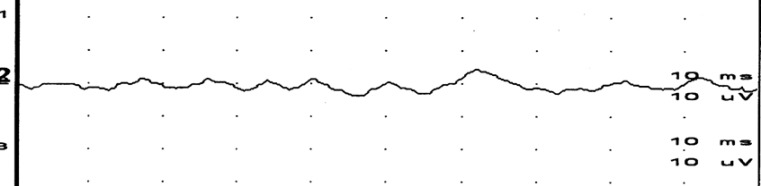
Fig. 3 An example of absence of vestibular evoked myogenic potentials formation.
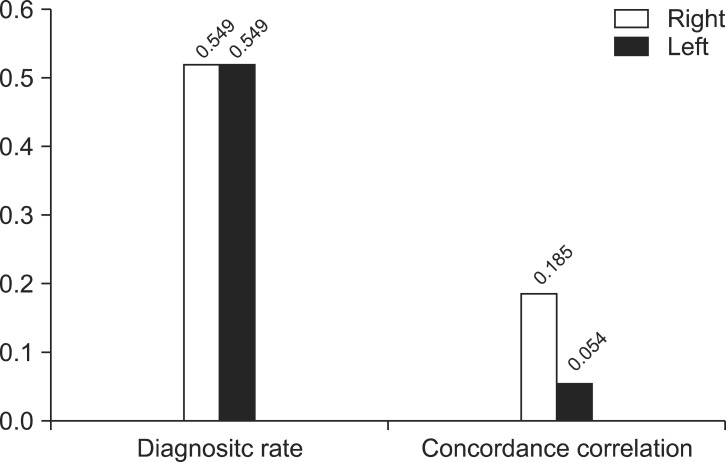
Fig. 4 In the case of defining as a disorder when any of the three diagnosis criteria (prolonged latency, shortened interpeak latency, and absence of vestibular evoked myogenic potentials formation) shows abnormality: diagnosis rates of both positions showed no significant differences in both sides but concordance correlation was low.
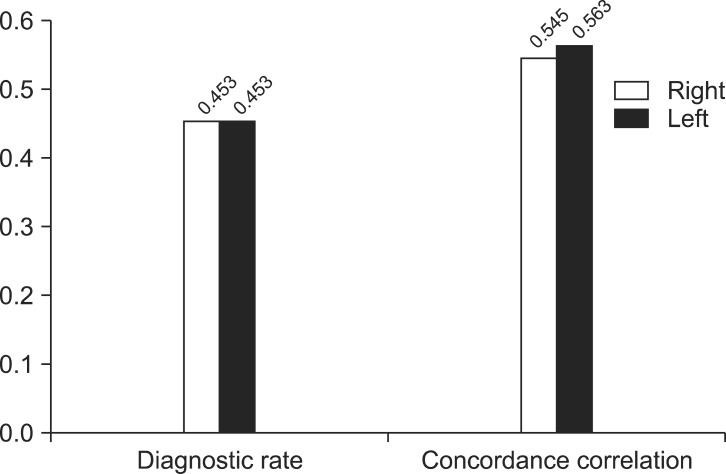
Fig. 5 In the case of defining disorder solely by prolonged latency: diagnosis rates of both positions showed no significant differences in both sides and concordance correlation was high.
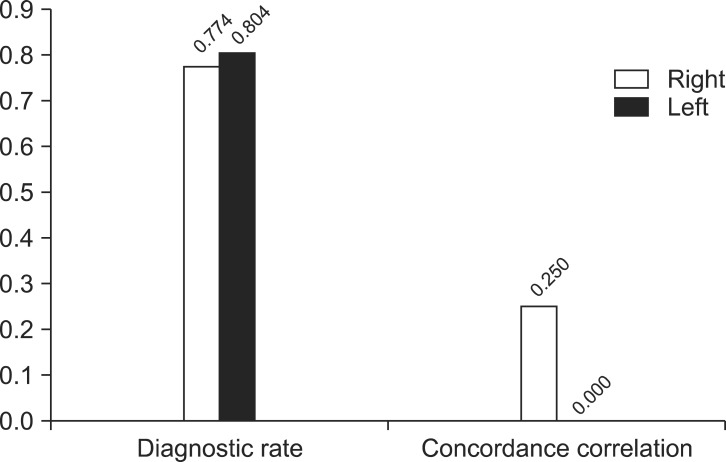
Fig. 6 In the case of defining disorder by shortened interpeak latency alone: diagnosis rates of both positions showed no significant differences in both sides but concordance correlation was low.
Reference
-
1. Tullio P. Das ohr und die entstehung der sprache und schrift. Berlin: Urban & Schwarzenberg;1929.2. Bickford RG, Jacobson JL, Cody DT. Nature of average evoked potentials to sound and other stimuli in man. Ann N Y Acad Sci. 1964; 112:204–223. PMID: 14188095.
Article3. Didier A, Cazals Y. Acoustic responses recorded from the saccular bundle on the eighth nerve of the guinea pig. Hear Res. 1989; 37:123–127. PMID: 2914808.
Article4. Ferber-Viart C, Dubreuil C, Duclaux R. Vestibular evoked myogenic potentials in humans: a review. Acta Otolaryngol. 1999; 119:6–15. PMID: 10219378.5. Colebatch JG, Halmagyi GM. Vestibular evoked potentials in human neck muscles before and after unilateral vestibular deafferentation. Neurology. 1992; 42:1635–1636. PMID: 1641165.
Article6. Mudduwa R, Kara N, Whelan D, Banerjee A. Vestibular evoked myogenic potentials: review. J Laryngol Otol. 2010; 124:1043–1050. PMID: 20519040.
Article7. Colebatch JG, Halmagyi GM, Skuse NF. Myogenic potentials generated by a click-evoked vestibulocollic reflex. J Neurol Neurosurg Psychiatry. 1994; 57:190–197. PMID: 8126503.
Article8. Murofushi T, Halmagyi GM, Yavor RA, Colebatch JG. Absent vestibular evoked myogenic potentials in vestibular neurolabyrinthitis: an indicator of inferior vestibular nerve involvement? Arch Otolaryngol Head Neck Surg. 1996; 122:845–848. PMID: 8703387.
Article9. Murofushi T, Curthoys IS. Physiological and anatomical study of click-sensitive primary vestibular afferents in the guinea pig. Acta Otolaryngol. 1997; 117:66–72. PMID: 9039484.
Article10. Kim JD, Goh EK, Lee YO, Kong SK, Cho KS, Chon KM. The effects of test positions and acoustic stimulations on the vestibular evoked myogenic potentials. J Korean Bal Soc. 2007; 6:21–28.11. Goh EK. Vestibular evoked myogenic potential. J Clin Otolaryngol Head Neck Surg. 2008; 19:13–17.
Article12. Lee SK, Cha CI, Jung TS, Park DC, Yeo SG. Age-related differences in parameters of vestibular evoked myogenic potentials. Acta Otolaryngol. 2008; 128:66–72. PMID: 17851962.
Article13. Ferber-Viart C, Duclaux R, Colleaux B, Dubreuil C. Myogenic vestibular-evoked potentials in normal subjects: a comparison between responses obtained from sternomastoid and trapezius muscles. Acta Otolaryngol. 1997; 117:472–481. PMID: 9288199.
Article14. Cody DT, Bickford RG. Averaged evoked myogenic responses in normal man. Laryngoscope. 1969; 79:400–416. PMID: 5776736.
Article15. Kim H, Cha CI, Byun JY, Moon JH, Hong SM, Kim KH. Clinical usefulness of VEMP(vestibular evoked myogenic potential) in the evaluation of dizzy patients. Korean J Otolaryngol-Head Neck Surg. 2003; 46:391–395.16. Wang CT, Young YH. Comparison of the head elevation versus rotation methods in eliciting vestibular evoked myogenic potentials. Ear Hear. 2006; 27:376–381. PMID: 16825887.
Article17. Park SH, Cha CI, Kim KH, Kim H, Hwang MG, Hong NP. The clinical significance of vestibular evoked myogenic potential evoked by click sound. Korean J Otolaryngol-Head Neck Surg. 2001; 44:1253–1258.18. Ahn YJ, Hong SK, Kim JS, Koo JW. Diagnostic value of vestibular evoked myogenic potential in acoustic neuroma. J Korean Bal Soc. 2007; 6:138–142.19. Matsuzaki M, Murofushi T, Mizuno M. Vestibular evoked myogenic potentials in acoustic tumor patients with normal auditory brainstem responses. Eur Arch Otorhinolaryngol. 1999; 256:1–4. PMID: 10065377.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Principle and Methodology of Vestibular Evoked Myogenic Potential
- The Effects of Test Positions and Acoustic Stimulations on the Vestibular Evoked Myogenic Potentials
- Vestibular-evoked myogenic potentials: principle and clinical findings
- Clinical Applications of Vestibular Evoked Myogenic Potentials in Vestibular Disorders
- Cervical Vestibular Evoked Myogenic Potential and Ocular Vestibular Evoked Myogenic Potential in Patients With Vestibular Neuritis and Acute Viral Labyrinthitis
