The Therapeutic Effect of Tibia Counter Rotator With Toe-Out Gait Plate in the Treatment of Tibial Internal Torsion in Children
- Affiliations
-
- 1Department of Physical Medicine and Rehabilitation, Yeungnam University College of Medicine, Daegu, Korea. xena2010@naver.com
- 2Medical Devices Clinical Trial Center, Yeungnam University, Daegu, Korea.
- 3Department of Rehabilitation Science, Graduate School, Daegu University, Gyeongsan, Korea.
- 4Korean Pedorthic Institute, Goyang, Korea.
- 5Department of Physical Therapy, Daegu Health College, Daegu, Korea.
Abstract
OBJECTIVE
To evaluate the therapeutic effect of a Tibia Counter Rotator (TCR) with toe-out gait plate (GP) upon tibial internal torsion by a comparative analysis of transmalleolar angle (TMA) and gait analysis with GP alone.
METHODS
Twenty participants with tibial internal torsion were recruited for this study. Each 10 participants were included in group A with TCR and GP application and in group B with GP application only. The TMA and the kinematic results were used for the evaluation of the therapeutic effects of orthoses.
RESULTS
Within each group, TMA showed a significant increase after treatment. Group A showed a continuous improvement up to six months, however, group B showed an improvement up to five months only. Group A showed a significantly higher correction effect than group B after treatment. Regarding kinematic data, both groups showed a significantly decreased mean ankle adduction angle after treatment. However, group A showed a significantly lower mean ankle adduction angle than group B after six months.
CONCLUSION
The group with TCR and GP showed a significantly better outcome and continued correction force compared to the group with GP only. Our results suggest that TCR with GP may be useful therapeutic orthoses for children with tibial internal torsion.
Keyword
Figure
-
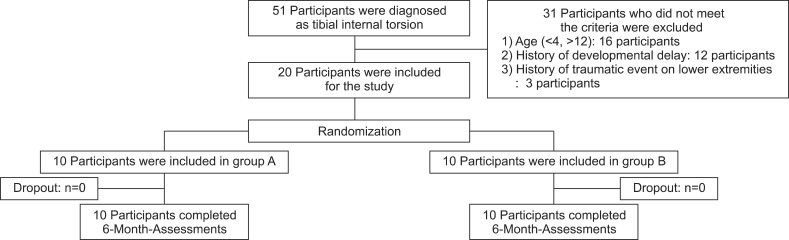
Fig. 1 Flowchart of subject selection. Fifty-one participants diagnosed as tibial internal torsion. Of 51 participants were 16 participants excluded who did not meet the age criterion: 12 participants were diagnosed as developmental delay and 3 participants had traumatic events on lower extremities during the study period. Finally, 20 participants were included in the study. A clinical coordinator unaware of the clinical data of participants randomized the subjects into two groups. Among 20 participants, 10 participants were included into group A with Tibial Counter Rotator (TCR) and toe-out gait plate (GP). The remaining 10 participants were included into group B with GP application only.
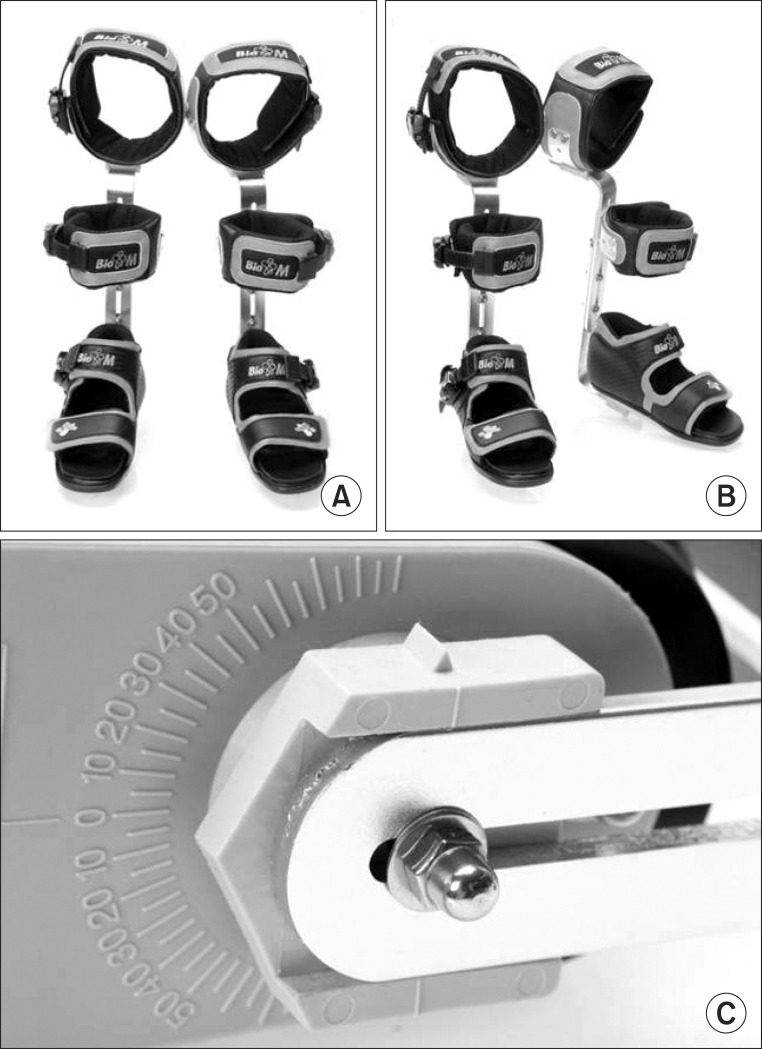
Fig. 2 Tibial Counter Rotator (TCR). (A) Anterior view, (B) oblique view, and (C) inferior view. TCR consisted of well-padded straps (Velcro), foot plate and metal brace (A, B). The initial setting angle was the end point of leg lateral motion with a flexed knee position. Foot plate angle was increased using units of 5° as the patients visited the foot clinic monthly (C). All participants were instructed to apply TCR with a flexed knee position during sleep for at least 3 hours a day.
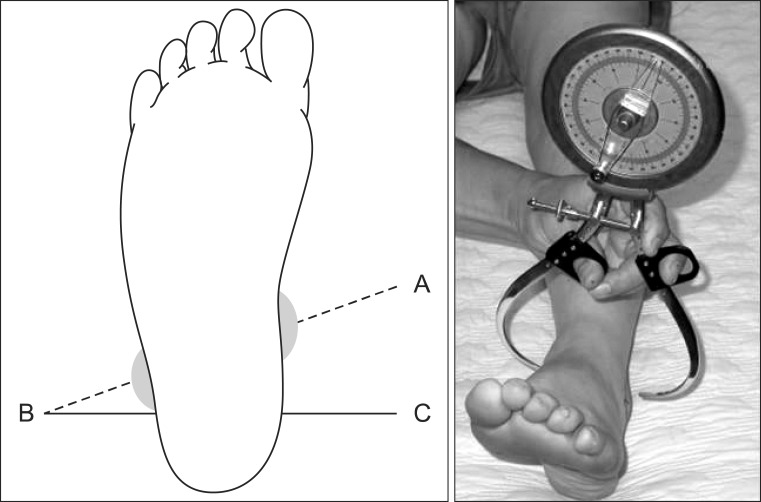
Fig. 3 Measurement of transmalleolar angle (TMA). TMA was measured using a gravity goniometer in the supine position after marking the medial malleolus of the tibia and lateral malleolus of the fibula while extending the knee to the coronal plane [5,6,8,9,18]. The negative value refers to the internal rotation of the tibia, whereas the positive value refers to the external rotation.
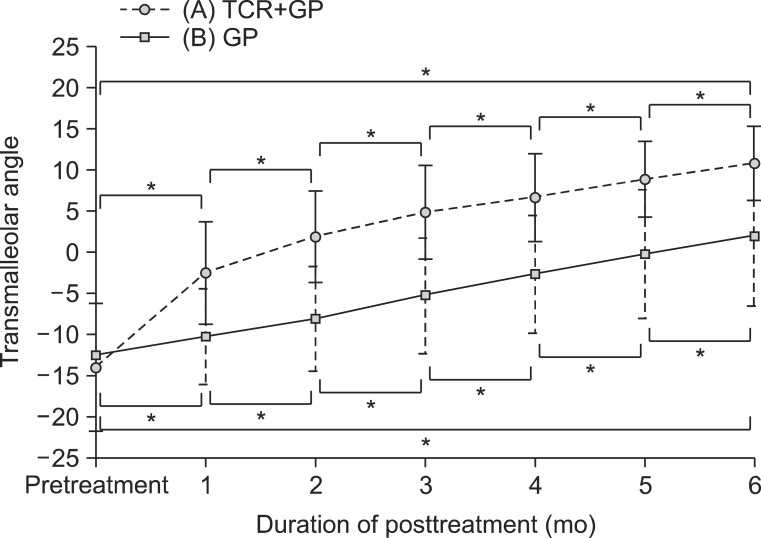
Fig. 4 Comparative results of transmalleolar angle within both groups. TCR, Tibial Counter Rotator; GP, toe-out gait plate. *p<0.05.
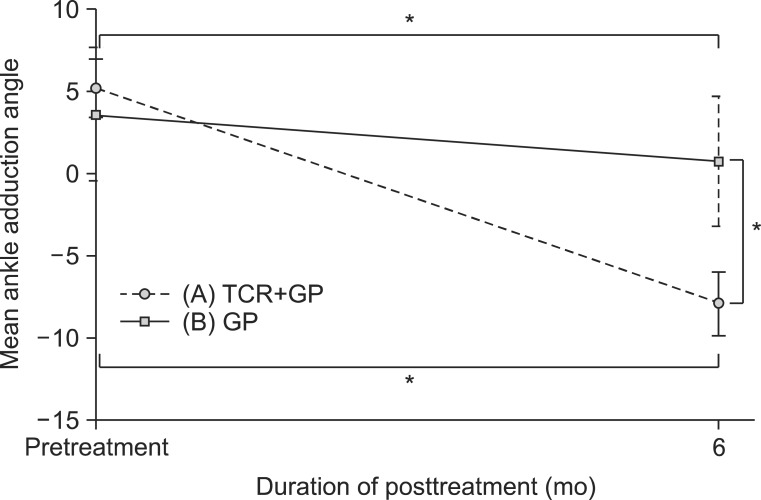
Fig. 5 Comparative results of mean foot ankle adduction angle in both groups. TCR, Tibial Counter Rotator; GP, toe-out gait plate. *p<0.05.
Reference
-
1. Song DH, Lee Y, Eun BL, Lee KJ, Kang SK, Vaq SG, et al. Usefulness of tibia counter rotator (TCR) for treatment of tibial internal torsion in children. Korean J Pediatr. 2007; 50:79–84.
Article2. Staheli LT, Corbett M, Wyss C, King H. Lower-extremity rotational problems in children: normal values to guide management. J Bone Joint Surg Am. 1985; 67:39–47. PMID: 3968103.
Article3. Thackeray C, Beeson P. In-toeing gait in children: a review of the literature. Foot. 1996; 6:1–4.
Article4. Jacquemier M, Glard Y, Pomero V, Viehweger E, Jouve JL, Bollini G. Rotational profile of the lower limb in 1319 healthy children. Gait Posture. 2008; 28:187–193. PMID: 18201887.
Article5. Valmassy R, Stanton B. Tibial torsion: normal values in children. J Am Podiatr Med Assoc. 1989; 79:432–435. PMID: 2778678.6. Valmassy RL. Biomechanical evaluation of the child. Clin Podiatry. 1984; 1:563–579. PMID: 6536409.7. Hutter CG Jr, Scott W. Tibial torsion. J Bone Joint Surg Am. 1949; 31A:511–518. PMID: 18153894.
Article8. McDonough MW. Angular and axial deformities of the legs of children. Clin Podiatry. 1984; 1:601–620. PMID: 6536411.9. Song DH, Eun BL, Park SH, Lee JY, Tockgo YC. Tibial torsion in children of the Jeju area. Korean J Pediatr. 2005; 48:75–80.10. Turner MS. The association between tibial torsion and knee joint pathology. Clin Orthop Relat Res. 1994; (302):47–51. PMID: 8168321.
Article11. Turner MS, Smillie IS. The effect of tibial torsion of the pathology of the knee. J Bone Joint Surg Br. 1981; 63B:396–398. PMID: 7263753.
Article12. Yagi T. Tibial torsion in patients with medial-type osteoarthrotic knees. Clin Orthop Relat Res. 1994; (302):52–56. PMID: 8168322.
Article13. Mabuchi A, Kitoh H, Inoue M, Hayashi M, Ishiguro N, Suzuki N. The biomechanical effect of the sensomotor insole on a pediatric intoeing gait. ISRN Orthop. 2012; 2012:1–5.
Article14. Redmond AC. An evaluation of the use of gait plate inlays in the short-term management of the intoeing child. Foot Ankle Int. 1998; 19:144–148. PMID: 9542984.
Article15. Bresnahan PJ, Lubert MA. The tibial torsion transformer. J Am Podiatr Med Assoc. 1992; 82:42–44. PMID: 1545370.
Article16. Lee SY, Jung YT, Lee SM. Effect of the tibia counter rotator orthosis for tibial internal torsion children: a preliminary study. J Korean Acad Rehabil Med. 2009; 33:470–476.17. Vanderwilde R, Staheli LT, Chew DE, Malagon V. Measurements on radiographs of the foot in normal infants and children. J Bone Joint Surg Am. 1988; 70:407–415. PMID: 3346265.
Article18. Lee SH, Chung CY, Park MS, Choi IH, Cho TJ. Tibial torsion in cerebral palsy: validity and reliability of measurement. Clin Orthop Relat Res. 2009; 467:2098–2104. PMID: 19159112.
Article19. Chambers C, Goode B. Variability in gait measurements across multiple sites. Gait Posture. 1996; 4:167.
Article20. Westhoff B, Hirsch MA, Hefter H, Wild A, Krauspe R. Wie reliable sind informationen aus der 3D-ganganalyse? Sportverletz Sportschaden. 2004; 18:76–79. PMID: 15164292.21. Weseley MS, Barenfeld PA, Eisenstein AL. Thoughts on in-toeing and out-toeing: twenty years' experience with over 5000 cases and a review of the literature. Foot Ankle. 1981; 2:49–57. PMID: 7030890.
Article22. Lang LM, Volpe RG. Measurement of tibial torsion. J Am Podiatr Med Assoc. 1998; 88:160–165. PMID: 9581433.
Article23. Abel MF, Sutherland DH, Wenger DR, Mubarak SJ. Evaluation of CT scans and 3-D reformatted images for quantitative assessment of the hip. J Pediatr Orthop. 1994; 14:48–53. PMID: 8113372.
Article24. Stuberg W, Temme J, Kaplan P, Clarke A, Fuchs R. Measurement of tibial torsion and thigh-foot angle using goniometry and computed tomography. Clin Orthop Relat Res. 1991; (272):208–212. PMID: 1934735.
Article25. Liu X, Kim W, Drerup B, Mahadev A. Tibial torsion measurement by surface curvature. Clin Biomech (Bristol, Avon). 2005; 20:443–450.
Article26. Lee S, Choi KS, Jeung IS, Lee JE, Yang SM, Lee SM. Physical examination and computed tomography in children with toe in gait. J Korean Acad Rehabil Med. 2011; 35:61–66.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effect of the Tibia Counter Rotator Orthosis for Tibial Internal Torsion Children: A Preliminary Study
- Usefulness of tibia counter rotator (TCR) for treatment of tibial internal torsion in children
- Relationship between Femoral Anteversion and Tibial Torsion in Intoeing Gait
- Physical Examination and Computed Tomography in Children with Toe in Gait
- Treatment of the Resistant Idiopathic Clubfoot with Toe-in Gait
