Efficacy of Tympanoplasty Without Mastoidectomy for Treating Chronic Otitis Media in Patients With Mastoid Cavity Opacification in Temporal Bone Computed Tomography Findings
- Affiliations
-
- 1Department of Otolaryngology, Ajou University School of Medicine, Suwon, Korea. yhc@ajou.ac.kr
- 2Department of Medical Sciences, Ajou University Graduate School of Medicine, Suwon, Korea.
- 3BK21 Plus Research Center for Biomedical Sciences, Ajou University Graduate School of Medicine, Suwon, Korea.
- KMID: 2407789
- DOI: http://doi.org/10.21053/ceo.2017.00878
Abstract
OBJECTIVES
Combined mastoidectomy is generally preferred to tympanoplasty alone when treating patients with chronic otitis media (COM), particularly when temporal bone computed tomography (TBCT) shows that the mastoid cavity contains opacification of soft tissue density. However, in cases with Eustachian tube dysfunction, a mastoid cavity volume may be a burden to its function. We hypothesized that tympanoplasty alone might be better than tympanoplasty combined with mastoidectomy because soft tissue in the mastoid cavity is a sequel to a protective physiological response. Thus, we explored the efficacy of tympanoplasty without mastoidectomy in COM patients exhibiting mastoid air cell opacification on TBCT.
METHODS
Between 2010 and 2014, a total of 33 patients, diagnosed with COM and with evidence of mastoid cavity opacification on TBCT, underwent tympanoplasty without mastoidectomy. All ears had been dry for ≥3 months before surgery. All procedures were performed by the same surgeon. We retrospectively analyzed the preoperative otoscopic findings, pre- and postoperative pure tone averages (PTAs; the mean of the values at 0.5, 1, 2, and 4 kHz), surgical procedures, and complications or recurrence.
RESULTS
Of the 33 patients, 28 (84.8%) exhibited hearing improvement after surgery. The mean pre- and postoperative PTAs were 46.9±21.2 dB and 29.4±17.0 dB, respectively (P < 0.001). The air-bone gap decreased from 25.7±10.7 dB to 10.3±8.7 dB (P < 0.001). Thirty-two patients (97.0%) did not develop any COM recurrence or cholesteatoma; one patient developed attic retraction of the tympanic membrane. Other minor complications were transient otorrhea caused by myringitis (two cases) and a pinpoint perforation (one case).
CONCLUSION
Tympanoplasty alone, i.e., without mastoidectomy, may adequately control COM, if it shows dry-up status for at least 3 months even though mastoid cavity opacification is detected in TBCT.
MeSH Terms
Figure
-
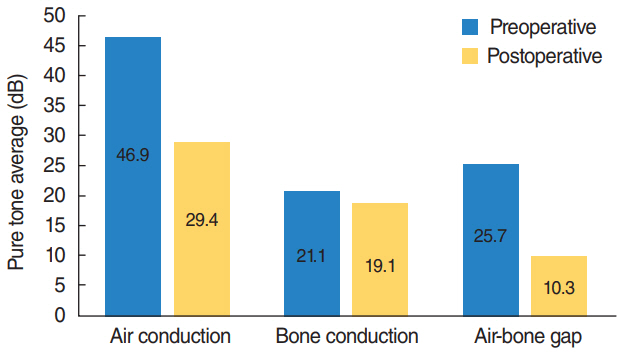
Fig. 1. Audiometric evaluation of the successful 28 patients. Both air conduction and the air-bone gap improved significantly.
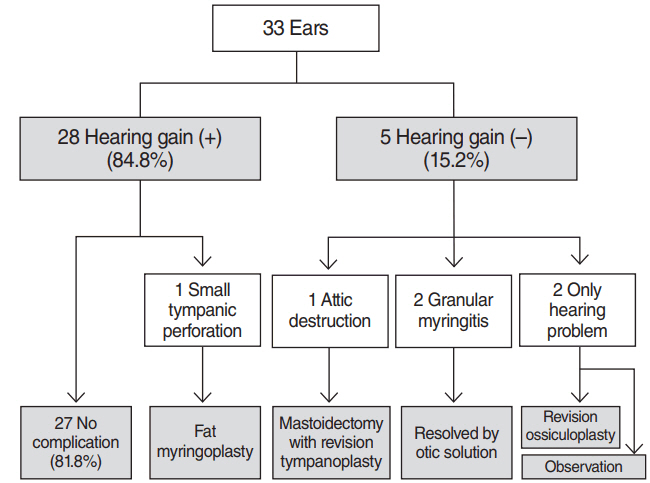
Fig. 2. Complications and their management after tympanoplasty. Mastoidectomy was performed on one patient because of progressive attic destruction after surgery. Overall, >80% of patients experienced better hearing outcomes without any complications.
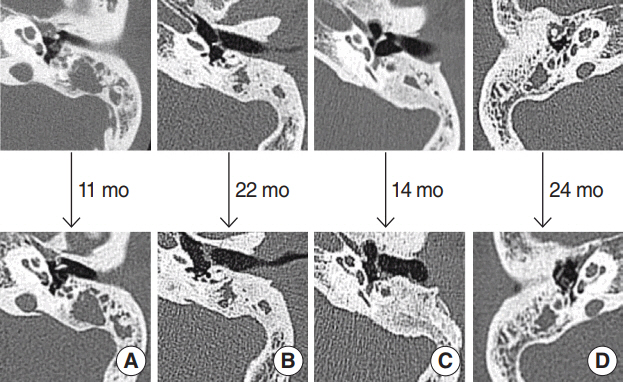
Fig. 3. No change in opacification was evident on follow-up temporal bone computed tomography of four patients. (A) A 22-year-old female: type I tympanoplasty, left. (B) A 47-year-old male: type III tympanoplasty, left. (C) A 42-year-old female: type III tympanoplasty, left. (D) A 52-year-old female: type I tympanoplasty, right.
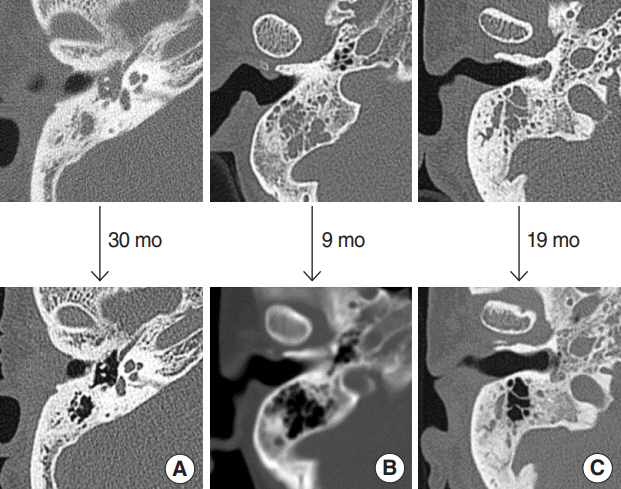
Fig. 4. Resolution of mastoid cavity haziness during post-tympanoplasty follow-up temporal bone computed tomography. (A) A 68- year-old male: type I tympanoplasty, right. (B) A 42-year-old female: type I tympanoplasty, right. (C) A 55-year-old female: type I tympanoplasty, right.
Reference
-
1. Brackmann DE, Shelton C, Arriaga MA. Otologic surgery. 1st ed. Philadelphia: W.B. Saunders;1994.2. Vartiainen E, Kansanen M. Tympanomastoidectomy for chronic otitis media without cholesteatoma. Otolaryngol Head Neck Surg. 1992; Mar. 106(3):230–4.
Article3. Mishiro Y, Sakagami M, Kondoh K, Kitahara T, Kakutani C. Long-term outcomes after tympanoplasty with and without mastoidectomy for perforated chronic otitis media. Eur Arch Otorhinolaryngol. 2009; Jun. 266(6):819–22.
Article4. Webb BD, Chang CY. Efficacy of tympanoplasty without mastoidectomy for chronic suppurative otitis media. Arch Otolaryngol Head Neck Surg. 2008; Nov. 134(11):1155–8.
Article5. O’Reilly BJ, Chevretton EB, Wylie I, Thakkar C, Butler P, Sathanathan N, et al. The value of CT scanning in chronic suppurative otitis media. J Laryngol Otol. 1991; Dec. 105(12):990–4.6. Leighton SE, Robson AK, Anslow P, Milford CA. The role of CT imaging in the management of chronic suppurative otitis media. Clin Otolaryngol Allied Sci. 1993; Feb. 18(1):23–9.
Article7. Takahashi H, Honjo I, Naito Y, Miura M, Tanabe M, Hasebe S, et al. Gas exchange function through the mastoid mucosa in ears after surgery. Laryngoscope. 1997; Aug. 107(8):1117–21.
Article8. Kumar V, Abbas AK, Aster JC. Robbins and Cotran pathologic basis of disease. 9th ed. Philadelphia: Elsevier Saunders;2015.9. Kim HJ. Classification and hearing result reporting guideline in chronic otitis media surgery. Korean J Otorhinolaryngol Head Neck Surg. 2006; Jan. 49(1):2–6.10. Hergils L, Magnuson B. Morning pressure in the middle ear. Arch Otolaryngol. 1985; Feb. 111(2):86–9.
Article11. Buckingham RA, Stuart DR, Geick MR, Girgis SJ, McGee TJ. Experimental evidence against middle ear oxygen absorption. Laryngoscope. 1985; Apr. 95(4):437–42.
Article12. Kanemaru S, Nakamura T, Omori K, Magrufov A, Yamashita M, Ito J. Regeneration of mastoid air cells in clinical applications by in situ tissue engineering. Laryngoscope. 2005; Feb. 115(2):253–8.
Article13. Wilkinson SL, Sahota RS, Constable JD, Harper F, Judd O. Does incidental mastoid opacification on computerized tomography necessitate referral to ENT? Laryngoscope. 2017; Dec. 127(12):2860–5.
Article14. Gwaltney JM Jr, Phillips CD, Miller RD, Riker DK. Computed tomographic study of the common cold. N Engl J Med. 1994; Jan. 330(1):25–30.
Article15. Lo AC, Nemec SF. Opacification of the middle ear and mastoid: imaging findings and clues to differential diagnosis. Clin Radiol. 2015; May. 70(5):e1–13.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Postoperative Mastoid Aeration Following Canal Wall Up Mastoidectomy according to Preoperative Middle Ear Disease: Analysis of Temporal Bone Computed Tomography Scans
- Clinical Analysis of Intact Bridge Mastoidectomy
- Comparison of Hearing Results by Type of Tympanoplasty with Mastoid Obliteration during Chronic Otitis Media Surgery
- The Effect of Mastoidectomy Combined with Tympanoplasty Type I on Postoperative Hearing in Chronic Otitis Media Patients Older than 65 Years
- Eustachian Tube Function and Mastoid Pneumatization as Prognostic Factors of Type 1 Tympanoplasty
