Clinical and Imaging Findings of Musculoskeletal Melioidosis in the Right Hip: A Case Report
- Affiliations
-
- 1Department of Radiology, Eulji University Hospital, Daejeon, Korea. tchun@eulji.ac.kr
- KMID: 2405724
- DOI: http://doi.org/10.3348/jksr.2018.78.3.212
Abstract
- Melioidosis is an infectious disease caused by a Gram-negative bacterium thought to be caused Burkholderia pseudomallei. This disease is endemic in tropical regions, but is not endemic and is rarely encountered in Korea. Nevertheless, the importance of early diagnosis of melioidosis is drawing substantial attention, due to its proliferation and the high mortality caused by the disease. Melioidosis can attack any organ, and manifests with a variety of symptoms. In particular, musculoskeletal melioidosis is rare and presents with nonspecific musculoskeletal symptoms. The imaging features of musculoskeletal melioidosis manifest a form of osteomyelitis or septic arthritis with soft tissue abscess or can mimic a bone tumor. This study describes the clinical and imaging findings of melioidosis involving the right femur and hip joint in a 64-year-old man.
MeSH Terms
Figure
-

Fig. 1. A 64-year-old melioidosis patient with right hip pain. A. Initial and 3 weeks follow-up radiography images including the right hip show no abnormal findings on soft tissue or bony structure. B. Whole body bone scan shows multifocal increased uptake in the greater and lesser trochanter of the right femur, and weak uptake in the femoral head. A 64-year-old melioidosis patient with right hip pain. C. MRI shows abnormal lesion on the right proximal femur. Fat-suppressed T2-weighted MRI shows heterogeneously high signal intensity and T1-weighted MRI and proton density-weighted MRI show heterogeneously low signal intensity in the inferior portion of the femoral head, neck, greater and lesser trochanter, and the proximal shaft of the femur. Some areas that showed high signal intensity on T2-weighted MRI did not show enhancement. These non-enhanced areas are thought to consist of necrotic tissues. Contrast enhancement is observed not only in bone but also in surrounding soft tissue and iliopsoas bursa. MRI = magnetic resonance imaging A 64-year-old melioidosis patient with right hip pain. D. Magnetic resonance image shows prominent synovial thickening and enhancement with increased joint effusion in the right hip joint.

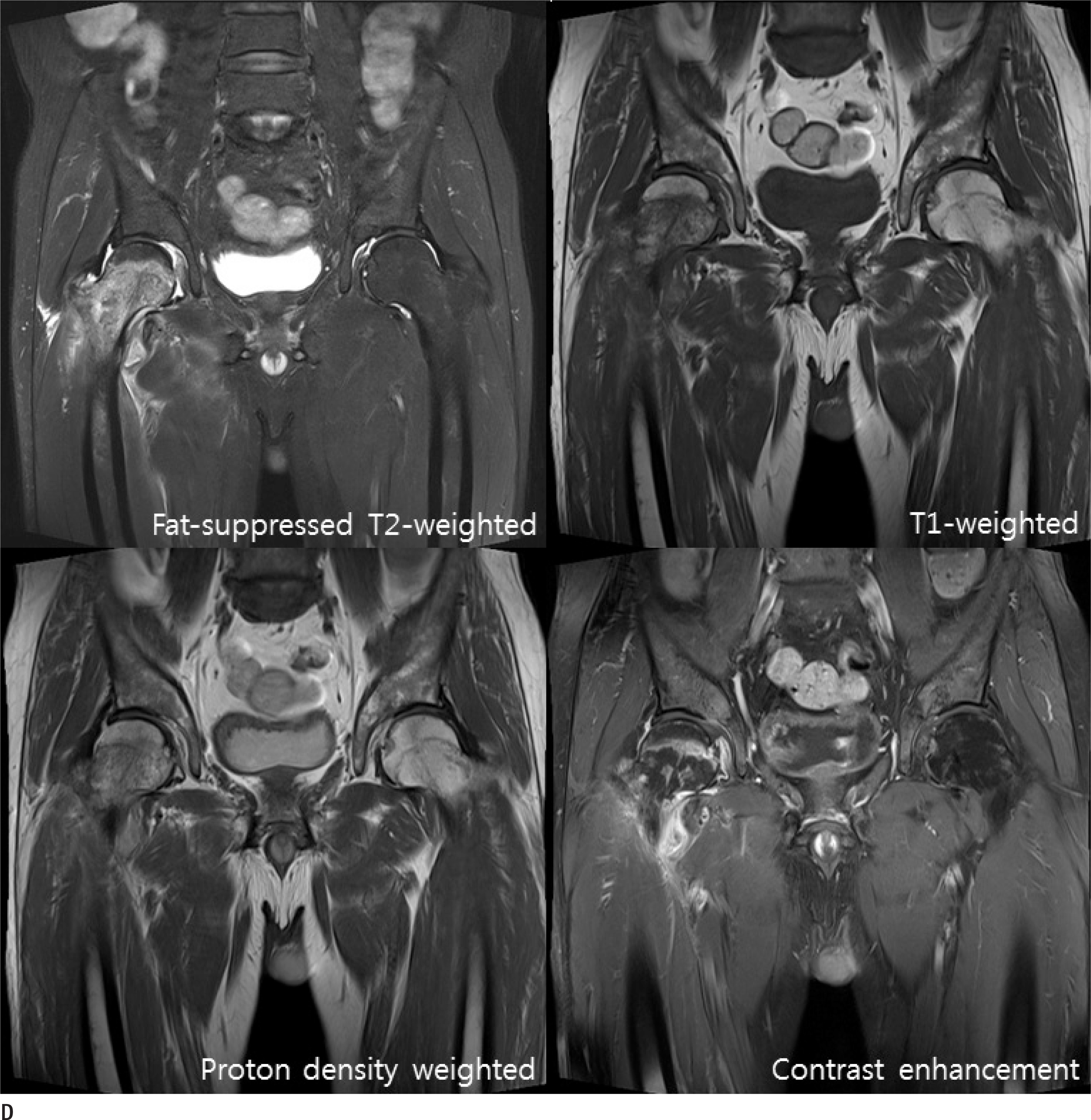

Fig. 1. A 64-year-old melioidosis patient with right hip pain. E. Positron emission tomography/computed tomography shows multifocal hypermetabolic lesion on the proximal shaft of the femur, femur neck, femoral head and iliopsoas bursa. F. Post-excisional biopsy radiography (left) shows fracture of the lesser trochanter of the right femur and an irregular shaped radiolucent area on the right proximal shaft of the femur. This is thought to be due to the excisional biopsy. Post-re-operative radiography (right) shows widened radiolucent area on the proximal shaft of the femur where the drainage catheter tip is located. This indicates that an abscess is formed in this radiolucent lesion.
Reference
-
References
1. Kim SW, Kwon GY, Kim B, Kwon D, Shin J, Bae GR. Imported melioidosis in South Korea: a case series with a literature review. Osong Public Health Res Perspect. 2015; 6:363–368.
Article2. Lim KS, Chong VH. Radiological manifestations of melioidosis. Clin Radiol. 2010; 65:66–72.
Article3. Muttarak M, Peh WC, Euathrongchit J, Lin SE, Tan AG, Lert-tumnongtum P, et al. Spectrum of imaging findings in melioidosis. Br J Radiol. 2009; 82:514–521.
Article4. Cheng AC, Currie BJ. Melioidosis: epidemiology, pathophysiology, and management. Clin Microbiol Rev. 2005; 18:383–416.
Article5. Kwon KY, Yoon SK. Characteristic of melioidosis and current status of infection in Korea. Public Health Wkly Rep. 2012; 5:10–12.6. Korea Centers for Disease Control and Prevention. Guideline for melioidosis prevention and control KCDC. Available at:. http://cdc.go.kr/CDC/notice/CdcKrTogether0302.jsp?menuIds=HOME001-MNU1154-MNU0005-MNU0088&cid=68797/. Published Jul 12, 2016. Accessed Mar 15,. 2017.7. Jain VK, Jain D, Kataria H, Shukla A, Arya RK, Mittal D. Melioidosis: a review of orthopedic manifestations, clinical features, diagnosis and management. Indian J Med Sci. 2007; 61:580–590.
Article8. Currie BJ, Ward L, Cheng AC. The epidemiology and clinical spectrum of melioidosis: 540 cases from the 20 year Darwin prospective study. PLoS Negl Trop Dis. 2010; 4:e900.
Article9. Raja NS, Scarsbrook C. Burkholderia pseudomallei causing bone and joint infections: a clinical update. Infect Dis Ther. 2016; 5:17–29.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Outcomes in Musculoskeletal Involvement of Burkholderia Pseudomallei Infection
- Musculoskeletal Applications of Elastography: a Pictorial Essay of Our Initial Experience
- Easy Way Out-Quick Interpretation of Musculoskeletal Radiographs: The Lower Extremity
- Epidemiological Aspects of Imported Melioidosis in Korea and Japan, 2011 to 2020
- Imported Melioidosis in South Korea: A Case Series with a Literature Review
