Conservative Treatment of Physeal Bar after Triradiate Cartilage Injury
- Affiliations
-
- 1Department of Orthopedic Surgery, Eulji University School of Medicine, Daejeon, Korea. cyh@eulji.ac.kr
- KMID: 2405401
- DOI: http://doi.org/10.4055/jkoa.2018.53.1.66
Abstract
- We report a patient who experienced no function problems during the 5-year follow-up after a conservative treatment for minimally displaced acetabular fracture that developed as a result of the formation of physeal bar. According to the computed tomography, triradiate cartilage was fractured and minimally displaced, which was identified as a Salter Harris type II physeal injury. A fracture of the anterior wall of the acetabulum was also observed. It was judged as a stable fracture, and conservative treatment was performed. On the follow-up x-ray, the physeal bar was formed in the damaged triradiate cartilage. At 5-year follow-up, physeal injury of the triradiate cartilage has influenced the acetabular growth, resulting in acetabular dysplasia, pelvic asymmetry, hypoplasia of pubis, and widening of the tear drop. However, anteversion and inclination of the injured acetabulum were similar with those of the contralateral side. Our patient also did not complain of any hip discomfort.
Keyword
Figure
-
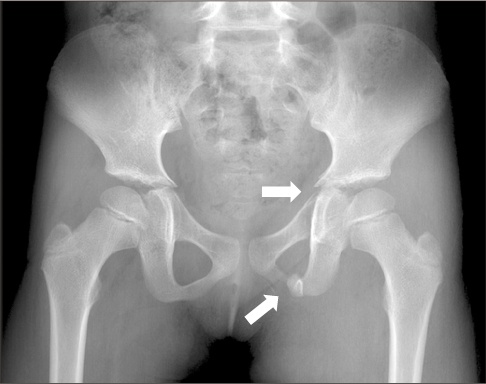
Figure 1 At both pelvic anteroposterior radiograph, left pubic ramus fracture with mild displacement is observed (white arrows).
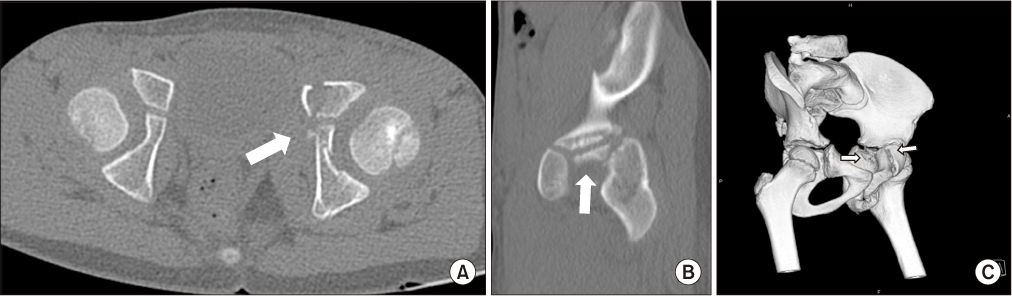
Figure 2 (A) It is an axial view of the computed tomography (CT). (B) It is a sagittal view of the CT of the left acetabulum. (C) On 3-dimensional CT, fracture line of anterior wall and fracture fragment of triradiate cartilage are observed (white arrows).
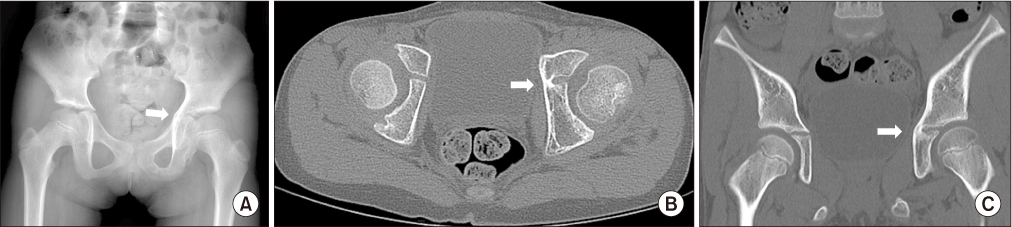
Figure 3 (A) A both pelvic anteroposterior radiograph taken at 1.5 years after injury. The physeal bar is formed on the axial view (B) and coronal view (C) of the computed tomography (white arrows).

Figure 4 A both pelvic anteroposterior radiographs taken at 5 years after injury.
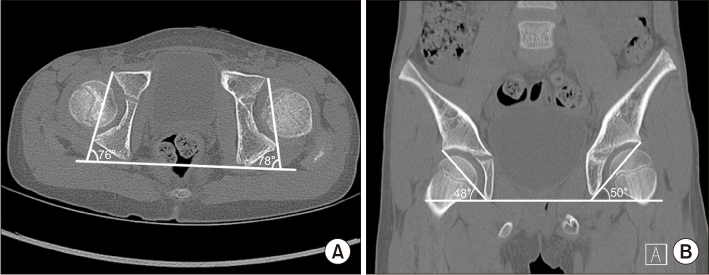
Figure 5 (A) At the final follow-up computed tomography (CT) axial view, right/left anteversion was measured as 14/12 degree. (B) At the final follow-up CT coronal view, right/left inclination was measured as 48/50 degree.
Reference
-
1. Watts HG. Fractures of the pelvis in children. Orthop Clin North Am. 1976; 7:615–624.
Article2. Bucholz RW, Ezaki M, Ogden JA. Injury to the acetabular triradiate physeal cartilage. J Bone Joint Surg Am. 1982; 64:600–609.
Article3. Trousdale RT, Ganz R. Posttraumatic acetabular dysplasia. Clin Orthop Relat Res. 1994; 305:124–132.
Article4. Spiguel L, Glynn L, Liu D, Statter M. Pediatric pelvic fractures: a marker for injury severity. Am Surg. 2006; 72:481–484.
Article5. Sharma UK, Basnyat A, Rijal K, Shrestha BK, Banskota B, Banskota AK. CT evaluation of pelvic and hip fractures. JNMA J Nepal Med Assoc. 2013; 52:586–590.6. Guerra MR, Braga SR, Akkari M, Santili C. Pelvic injury in childhood: what is its current importance? Acta Ortop Bras. 2016; 24:155–158.
Article7. Gänsslen A, Hildebrand F, Heidari N, Weinberg AM. Acetabular fractures in children: a review of the literature. Acta Chir Orthop Traumatol Cech. 2013; 80:10–14.8. Rodrigues KF. Injury of the acetabular epiphysis. Injury. 1973; 4:258–260.
Article9. Ponseti IV. Growth and development of the acetabulum in the normal child. Anatomical, histological, and roentgenographic studies. J Bone Joint Surg Am. 1978; 60:575–585.
Article10. Tavares JO. Modified Pemberton acetabuloplasty for the treatment of congenital hip dysplasia. J Pediatr Orthop. 2004; 24:501–507.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Treatment of Partial Closure of Growth Plate: Physeal Bar Resection and Free Fat Graft
- Prognostic Factors of Physeal Bar Resection and Fat Graft Interposition in the Treatment of Partial Physeal Arrest
- Physeal Defect Model of Rabbit's Tibia : Conventional Curettage vs Box Osteotome Method
- Treatment of Peterson classification Type VI of Physeal Injury in Ankle Joint: 2 cases report
- The Role of Y and Greater Trochanteric Growth Cartilage upon the Acetabular Development of Rabbits: An Experimental Study
