A Case of General Congenital Fibrosis Syndrome With A-pattern Strabismus
- Affiliations
-
- 1Department of ophthalmology, Maryknoll Hospital, Pusan, Korea. kris9352@hanmail.net
Abstract
-
PURPOSE: To report a case of general congenital fibrosis syndrome with A-pattern strabismus, bilateral ptosis and hypotropia.
CASE SUMMARY
A six-year-old girl was presented with severe bilateral ptosis and esodeviation of the left eye since birth. No levator action was presented and her chin was elevated at an angle of 25 degrees. In both eyes, an abduction defect was observed, and no vertical movement was presented. There was a left esotropia of 20 prism diopters (PD) and bilateral hypotropia of 35PD. There was an A-pattern strabismus that presents convergence movements during attempts to look upward, and orthotropia during attempts to look downward. Diagnosed as general congenital fibrosis syndrome with A-pattern esotropia, bilateral ptosis and hypotropia, bilateral inferior rectus muscle recessions were performed. After the operation, chin elevation and hypotropia in both eyes were corrected and exodeviation increased. Thus, orthotropia was observed in the primary position, and an A-pattern strabismus occurred with an exotropia of 15PD on the downgaze.
CONCLUSIONS
A congenital fibrosis syndrome with an A-pattern strabismus was reported for the first time by the authors. On decisions concerningsurgical amounts of horizontal deviation, exodeviation should be considered to increase after bilateral inferior rectus muscle recessions.
Figure
-

Figure 1. (A) Preoperative photograph shows bilateral ptosis and chin elevation. (B) Bell’s phenomenon was absent.

Figure 2. Preoperative photograph shows A-pattern esotropia that presents convergence movements on attemptsto look upward, a left esotropia of 20PD in the primary position, and orthotropia on attempts to look downward. Bilateral hypotropia of 35PD with no vertical movement, and abduction defect of both eyes were observed.
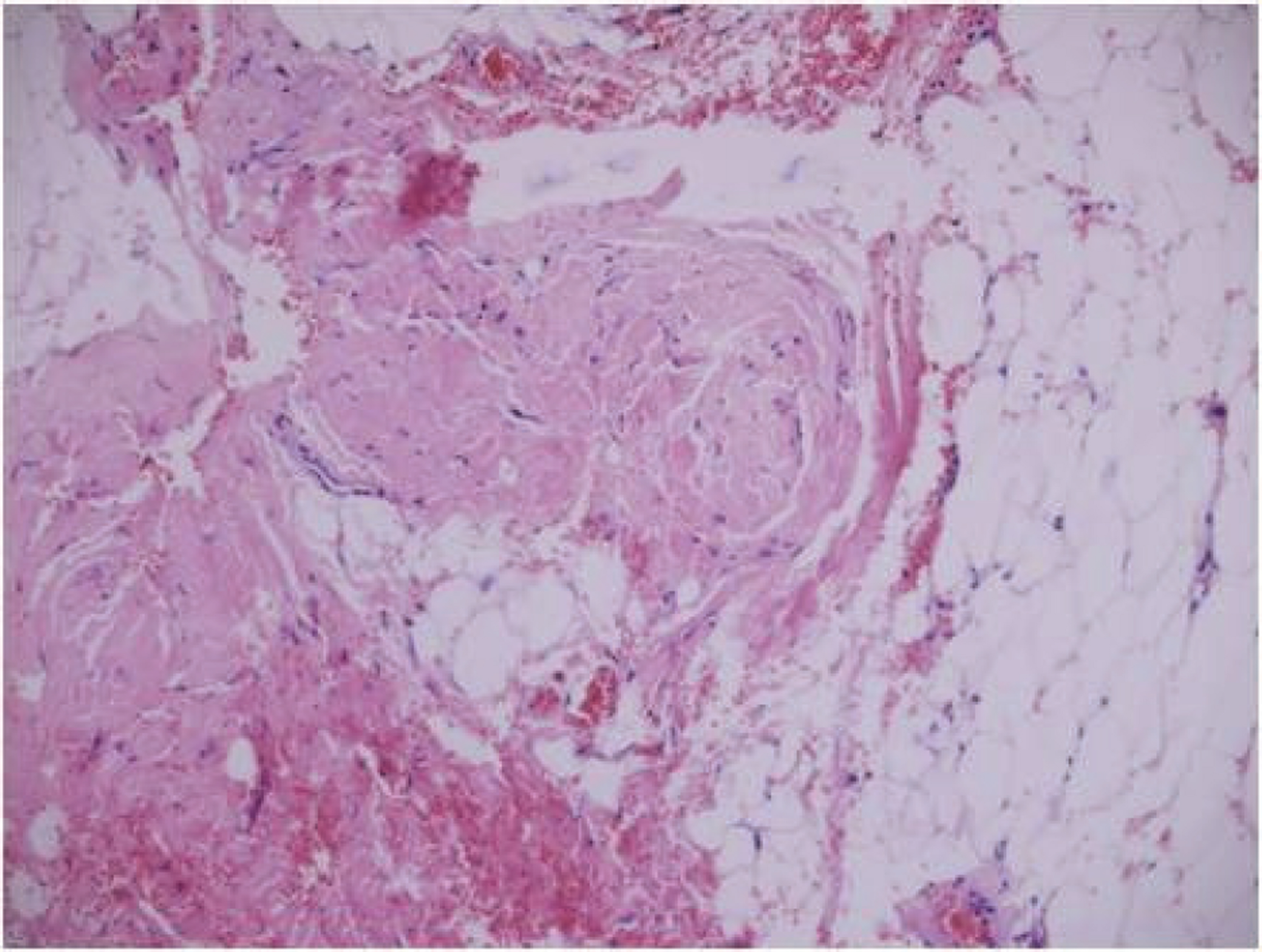
Figure 3. Light microscopic findingsof the inferior rectus muscle biopsy shows total displacement of muscle fibersby collagen fibers and fat (Masson-trichrome stain, ×200).

Figure 4. The postoperative 2-month photograph shows A-pattern strabismus that presents orthophoria in the primary position, an esotropia of 30PD in upgaze and an exotropia of 15PD in downgaze by increased postoperative exodeviation.
Reference
-
References
1. Apt L, Axelrod RN. Generalized fibrosis of the extraocular muscles. Am J Ophthalmol. 1978; 85:822–9.
Article2. Baumgarten M. Erfrahrugen uber den Strabismus und die Muskeldurchschneidung am Auge in physiologischpatho- logischer und therapeutischer Beziehung. Monatsschr Med Augenheilked Chir. 1840; 3:447–99.3. Brown HW. Congenital structural muscle abnormalities. Allen JH, editor. Strabismus Ophthalmic Symposium. St. Lousis, CV Mosby;1950. p. 205–36.4. Harley RD, Rodrigues MM, Crowford JS. Congenital fibrosis of the extraocular muscles. J Pediatr Opthalmol strabismus. 1978; 15:346–58.
Article5. Fells P, Waddell E, Rodrigues M. Progressive, exaggerated A-pattern strabismus with presumed fibrosis of the extraocular muscles. Reinecke RD, editor. Strabismus II. Proceedings of the Fourth Meeting at the International Strabisological Association. Oct. 25-29 1982, Asilomar, CA. Orlando: Grune & Stratton;1984. p. 335–42.6. Parks MM. Ocular Motility and Strabismus. Fibrosis syndrome. Hargerstown: Harper & Low;1975. p. 170–2.
Article7. Laughlin RC. Congenital fibrosis of the extrocular muscles. Am J Ophthalmol. 1956; 41:432–8.8. Von Noorden GK. Congenital hereditary ptosis with inferior rectus fibrosis. Arch Ophthalmol. 1970; 83:378–80.
Article9. Sugawara M, Awaya A, Makima A. . Studies on seven cases of general fibrosis syndrome. Anatomical anomaly of the extrocular muscle and their surgical correction. Nippon Ganka Gakkai Zasshi. 1982; 86:657.10. Traboulsi EI, Jaafar MS, Kattan HM. . Congenital fibrosis of the extraocular muscles: Report of 24 cases illustrating the clinical spectrum and surgical management. Am Orthopt J. 1993; 43:45–53.
Article11. Rosenbaum AL, Santiago AP. Clinical strabismus management. Philadelphia: Saunders;1999. p. 364.12. Engle EX, Goumnerov BC, McKeown CA. . Oculomotor nerve and muscle abnormalities in congenital fibrosis of the extraocular muscles. Ann Neurol. 1997; 41:314–25.
Article13. Brodsky MC. Hereditary external ophthalmoplegia, synergistic divergence, jaw winking, and oculocutaneous hypopig- mentation: a congenital fibrosis syndrome caused by deficient innervation to extraocular muscles. Ophthalmology. 1998; 105:717–25.14. Hartle RW, Katowitz JA, Young TL. . Congenital unilateral fibrosis, blepharoptosis, and enophthalmos syndrome. Ophthalmology. 1992; 99:347–55.
Article15. Von Noorden GK. Binocular vision and Ocular motility. 6th. St. Louis: CV Mosby;2002. –476.16. Ferre J. Congenital fibrosis of the extraocular muscles. Ophthalmology. 1996; 103:1517–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Divergent Strabismus Fixus
- Clinical Study of A-V Pattern Strabismus in Korea
- Surgical Correction of Lid Retraction with a Silicone Sponge in Congenital Fibrosis of the Extraocular Muscles
- Four Cases of Strabismus presenting after Cataract Surgery
- Clinical Features of Patients over the Age of 60 Years Who Have Undergone Strabismus Surgery
