J Korean Ophthalmol Soc.
2008 Dec;49(12):1929-1934.
Comparison of Silicone Oil Removal Using 23-Gauge and 20-Gauge System for Pars Plana Vitrectomy
- Affiliations
-
- 1Department of Ophthalmology, KyungHee University College of Medicine, Seoul, Korea. hwkwak@khmc.or.kr
Abstract
-
PURPOSE: The purpose of this study was to compare the clinical results of silicone oil removal using a 23-gauge transconjunctival sutureless pars plana vitrectomy (TSVS) and the 20-gauge pars plana vitrectomy (PPV) system and to evaluate the clinical value of 23-guage PPV system in silicone oil removal.
METHODS
Eight eyes of 8 patients who received removal of silicone oil using the 23-gauge TSVS and 6 eyes of 6 patients using the 20-gauge PPV system were included in this study. The total operation time, silicone oil removal time, intraoperative and postoperative advantages, shortcomings, and complications were compared.
RESULTS
The operation time and silicone oil removal time were 44.6+/-14.1 minutes, 42.7+/-10.5 minutes and 2.0+/-0.9 min/cc, 1.4+/-0.6 min/cc when silicone oil removal was performed using 23-gauge TSVS and 20-gauge PPV system, respectively. They were not significantly different (p=0.80, 0.22). Attention for the complete removal of the oil is necessary because of the intraocular trocar length when the 23-gauge TSVS is used. There were no complications except transient hypotonies (2 eyes), transient hypertonies (2 eyes) in the 23-gauge system and transient hypertonies (2 eyes) in the 20-gauge system.
CONCLUSIONS
The operation time for silicone oil removal using the 23-gauge TSVS was not different than that of the 20-gauge PPV system and can be performed safely without any particular complications. Care and precautionary measures are needed in order to remove silicone oil completely.
Keyword
Figure
-

Figure 1 . The photograph of silicone removal using 23-gauge vitrectomy system in a patient with proliferative diabetic retinopathy patient.
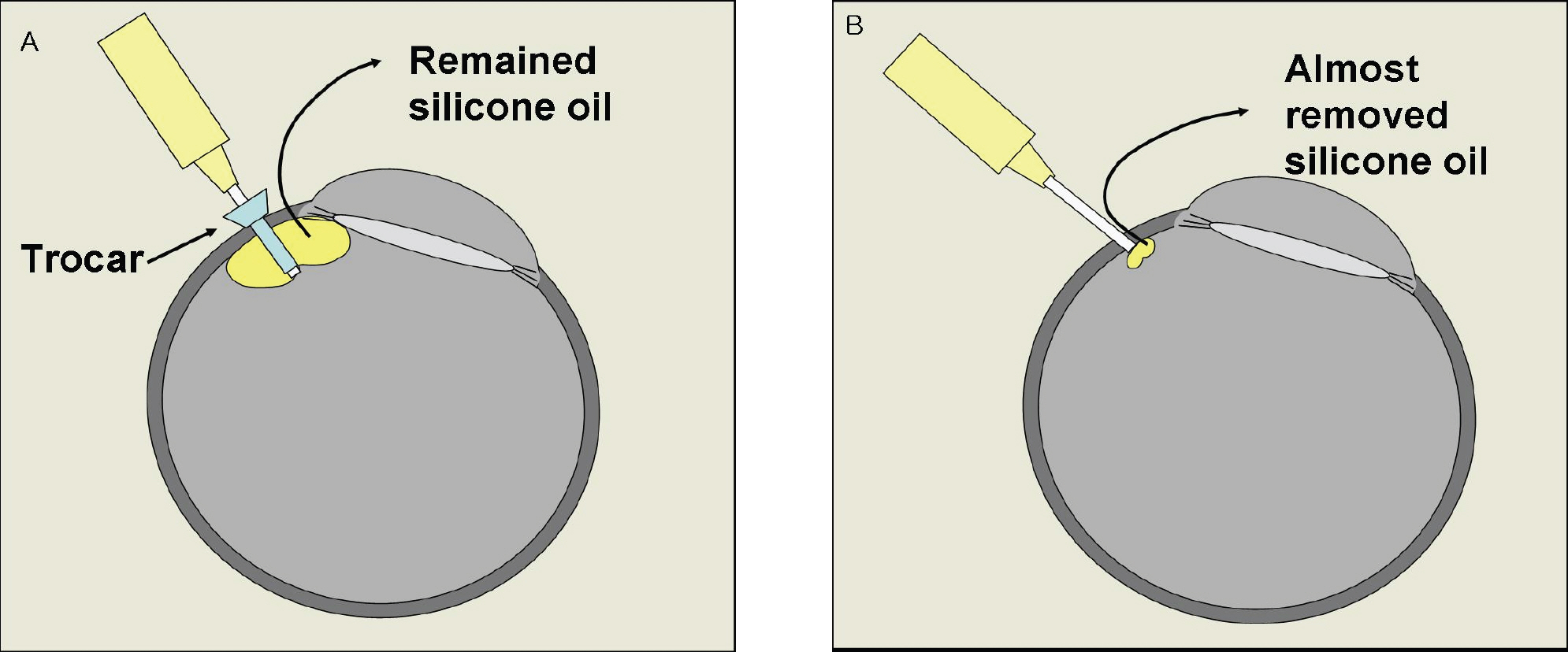
Figure 2 . Shortcoming of silicone removal using 23-gauge vitrectomy system (A) compared with 20-gauge vitrectomy system (B). In 23-gauge system, we need some attentions to remove silicone oil completely because of the intraocular trocar length but we can remove oil nearly completely by pulling the needle in 20-gauge system.
Reference
-
References
1. Casswell AG, Gregor ZJ. Silicone oil removal. II. Operative and postoperative complications. Br J Ophthalmol. 1987; 71:898–902.
Article2. Chen JC. Sutureless pars plana vitrectomy through self-sealing sclerotomies. Arch Ophthalmol. 1996; 114:1273–5.
Article3. Milibak T, Suveges I. Complications of sutureless pars plana vitrectomy through self-sealing sclerotomies. Arch Ophthalmol. 1998; 116:119.4. Kwok AK, Tham CC, Lam DS. . Modified sutureless sclerotomies in pars plana vitrectomy. Am J Ophthalmol. 1999; 127:731–3.
Article5. Schmidt J, Nietgen GW, Brieden S. Self-sealing, sutureless sclerotomy in pars plana vitrectomy in German. Klin Monatsbl Augenheilkd. 1999; 215:247–51.6. Jackson T. Modified sutureless sclerotomies in pars plana vitrectomy. Am J Ophthalmol. 2000; 129:116–7.
Article7. Assi AC, Scott RA, Charteris DG. Reversed self-sealing parsplana sclerotomies. Retina. 2000; 20:689–92.8. Rahman R, Rosen PH, Riddell C, Towler H. Self-sealing sclerotomies for sutureless pars plana vitrectomy. Ophthalmic Surg Lasers. 2000; 31:462–6.
Article9. Theelen T, Verbeek AM, Tilanus MA, van den Biesen PR. A novel technique for self-sealing, wedge-shaped pars plana sclerotomies and its features in ultrasound biomicroscopy and clinical outcome. Am J Ophthalmol. 2003; 136:1085–92.
Article10. Yanyali A, Celik E, Horozoglu F, Nohutcu AF. Corneal topographic changes after transconjunctival (25-gauge) sutureless vitrectomy. Am J Ophthalmol. 2005; 140:939–41.
Article11. Lakhanpal RR, Humayun MS, de Juan E Jr. . Outcomes of 140 consecutive cases of 25-gauge transconjunctival surgery for posterior segment disease. Ophthalmology. 2005; 112:817–24.
Article12. Meyer CH, Rodrigues EB, Schmidt JC. . Sutureless vitrectomy surgery. Ophthalmology. 2003; 110:2427–8.
Article13. Lam DS, Yuen CY, Tam BS. . Sutureless vitrectomy surgery. Ophthalmology. 2003; 110:2428–9.
Article14. Kapran Z, Acar N. Removal of silicone oil with 25-gauge transconjunctival sutureless vitrectomy system. Retina. 2007; 27:1059–64.
Article15. Cibis PA, Becker B, Okun E, Canaan S. The use of liguid silicone in retinal detachment surgery. Arch Ophthalmol. 1962; 68:590–9.16. Lucke K, Laqua H. Silicone oil in the treatment of complicated retinal detachment. 1st. Vol. 1. Berlin, New York: Springer;1990. p. 121.
Article17. Bodanowitz S, Kir N, Hesse L. Silicone oil for recurrent vitreous hemorrhage in previously vitrectomized diabetic eyes. Ophthalmologica. 1997; 211:219–22.
Article18. Hoerauf H, Roider J, Bopp S. . Endotamponade with silicone oil in severe proliferative retinopathy with attached retina. Ophthalmologe. 1995; 92:657–62.19. Riedel KG, Gabel VP, Neubauer L. . Intravitreal silicone oil injection: complications and treatment of 415 consecutive patients. Graefes Arch Clin Exp Ophthalmol. 1990; 228:19–23.
Article20. Eller AW, Gardner TW, D'Antonio JA. A survey of intraocular silicone oil use in the united states. Ophthalmology. 1992; 99:1174–6.
Article21. Oh TS, Kim SY. Complications associated with intravitreal silicone oil injection. J Korean Ophthalmol Soc. 1993; 34:1012–22.22. Pearson RV, McLeod D, Gregor ZJ. Removal of silicone oil following diabetic vitrectomy. Br J ophthalmol. 1993; 77:204–9.
Article23. Ekcardt C. Transconjunctival sutureless 23-gauze vitrectomy. Retina. 2005; 25:208–11.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Initial Experience With 20-Gauge Transconjunctival Sutureless Vitrectomy Using Conventional Instruments
- Sclerotomy-related Retinal Breaks in Vitrectomy for Proliferative Diabetic Retinopathy: 20- vs 23-Gauge Systems
- Hemorrhagic Retinal Macrocyst with Retinal Detachment
- Surgical Outcome and Significance of Silicone Oil Tamponade for Inferior Rhegmatogenous Retinal Detachment
- Comparison Between 20-Gauge and 23-Gauge Vitrectomy System in Primary Vitrectomy for Rhegmatogenous Retinal Detachment
