J Pathol Transl Med.
2018 Jan;52(1):21-27. 10.4132/jptm.2016.06.17.
Comparison of the Classical Method and SEE-FIM Protocol in Detecting Microscopic Lesions in Fallopian Tubes with Gynecological Lesions
- Affiliations
-
- 1Department of Pathology, Zeynep Kamil Maternity and Pediatric Research and Training Hospital, Istanbul, Turkey.
- 2Department of Obstetrics and Gynecology, Zeynep Kamil Maternity and Pediatric Research and Training Hospital, Istanbul, Turkey. pataraa96@gmail.com
- KMID: 2403254
- DOI: http://doi.org/10.4132/jptm.2016.06.17
Abstract
- BACKGROUND
The objective of this study was to compare the classical method and Sectioning and Extensively Examining the Fimbriated End Protocol (SEE-FIM) in detecting microscopic lesions in fallopian tubes with gynecological lesions.
METHODS
From a total of 1,118 cases, 582 with various parts of both fallopian tubes sampled in three-ring-shape sections and 536 sampled with the SEE-FIM protocol were included in this study. Pathological findings of cases with endometrial carcinoma, non-uterine pelvic malignant tumor, ovarian borderline tumors, premalignancy, and benign lesions were compared.
RESULTS
We detected two tubal infiltrative carcinomas among 40 uterine endometrioid adenocarcinomas, 15 serous tubal intraepithelial carcinomas in 39 non-uterine pelvic serous high-grade carcinoma cases, seven papillary tubal hyperplasias in 13 serous borderline tumor cases, and 11 endometriotic foci and four adenomatoid tumors among all cases sampled with the SEE-FIM protocol. Using the classical method, we detected only one serous tubal intraepithelial carcinoma in 113 non-uterine pelvic serous high-grade carcinoma cases and two papillary tubal hyperplasia cases in 31 serous borderline tumors. We did not identify additional findings in 185 uterine endometrioid carcinoma cases, and neither endometriotic focus nor adenomatoid tumor was shown in other lesions by the classical method.
CONCLUSIONS
Benign, premalignant, and malignant lesions can possibly be missed using the classical method. The SEE-FIM protocol should be considered especially in cases of endometrial carcinoma, nonuterine pelvic serous cancers, or serous borderline ovarian tumors. For other lesions, at least a detailed examination of the fimbrial end should be undertaken.
MeSH Terms
Figure
-
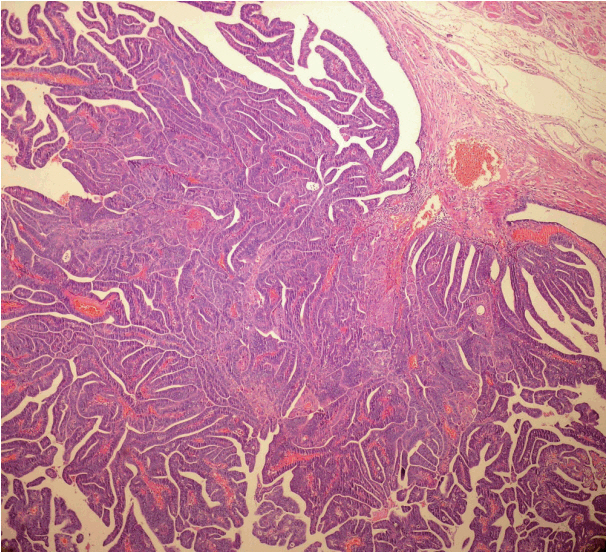
Fig. 1. Polypoid infiltrative endometrioid carcinoma extending to the tubal lumen.
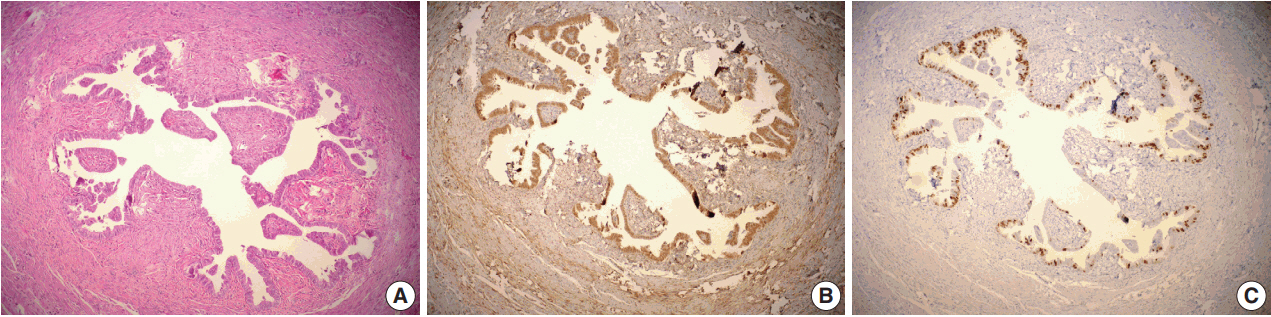
Fig. 2. Serous tubal intraepithelial carcinoma (A), positive immunostaining for p53 (B), and for Ki-67 (C).

Fig. 3. Papillary tubal hyperplasia. Small rounded clusters of tubal epithelial cells and small papillae associated with psammoma bodies.
Reference
-
1. Carcangiu ML, Peissel B, Pasini B, Spatti G, Radice P, Manoukian S. Incidental carcinomas in prophylactic specimens in BRCA1 and BRCA2 germ-line mutation carriers, with emphasis on fallopian tube lesions: report of 6 cases and review of the literature. Am J Surg Pathol. 2006; 30:1222–30.2. Yates MS, Meyer LA, Deavers MT, et al. Microscopic and early-stage ovarian cancers in BRCA1/2 mutation carriers: building a model for early BRCA-associated tumorigenesis. Cancer Prev Res (Phila). 2011; 4:463–70.3. Kurman RJ, Shih IM. Molecular pathogenesis and extraovarian origin of epithelial ovarian cancer: shifting the paradigm. Hum Pathol. 2011; 42:918–31.4. Kurman RJ, Vang R, Junge J, Hannibal CG, Kjaer SK, Shih IM. Papillary tubal hyperplasia: the putative precursor of ovarian atypical proliferative (borderline) serous tumors, noninvasive implants, and endosalpingiosis. Am J Surg Pathol. 2011; 35:1605–14.5. Seidman JD, Sherman ME, Bell KA, Katabuchi H, O’Leary TJ, Kurman RJ. Salpingitis, salpingoliths, and serous tumors of the ovaries: is there a connection? Int J Gynecol Pathol. 2002; 21:101–7.
Article6. Mehrad M, Ning G, Chen EY, Mehra KK, Crum CP. A pathologist’s road map to benign, precancerous, and malignant intraepithelial proliferations in the fallopian tube. Adv Anat Pathol. 2010; 17:293–302.
Article7. Rosai J. Rosai and Ackerman’s surgical pathology. St. Louis: Mosby Elsevier;2011.8. Kurman RJ, Hedrick Ellenson L, Ronnett BM. Blaustein’s pathology of the female genital tract. New York: Springer-Verlag;2011.9. Longacre TA, Oliva E, Soslow RA; Association of Directors of Anatomic and Surgical Pathology. Recommendations for the reporting of fallopian tube neoplasms. Hum Pathol. 2007; 38:1160–3.
Article10. Medeiros F, Muto MG, Lee Y, et al. The tubal fimbria is a preferred site for early adenocarcinoma in women with familial ovarian cancer syndrome. Am J Surg Pathol. 2006; 30:230–6.
Article11. Bloss JD, Liao SY, Buller RE, et al. Extraovarian peritoneal serous papillary carcinoma: a case-control retrospective comparison to papillary adenocarcinoma of the ovary. Gynecol Oncol. 1993; 50:347–51.
Article12. Kuhn E, Kurman RJ, Sehdev AS, Shih IM. Ki-67 labeling index as an adjunct in the diagnosis of serous tubal intraepithelial carcinoma. Int J Gynecol Pathol. 2012; 31:416–22.
Article13. Yemelyanova A, Vang R, Kshirsagar M, et al. Immunohistochemical staining patterns of p53 can serve as a surrogate marker for TP53 mutations in ovarian carcinoma: an immunohistochemical and nucleotide sequencing analysis. Mod Pathol. 2011; 24:1248–53.14. Culton LK, Deavers MT, Silva EG, Liu J, Malpica A. Endometrioid carcinoma simultaneously involving the uterus and the fallopian tube: a clinicopathologic study of 13 cases. Am J Surg Pathol. 2006; 30:844–9.15. Kulac I, Usubutun A. Microscopic lesions of fallopian tubes in endometrioid carcinoma of the endometrium: How effective are the macroscopic tubal sampling techniques? J Gynecol Oncol. 2013; 24:114–9.
Article16. Przybycin CG, Kurman RJ, Ronnett BM, Shih IM, Vang R. Are all pelvic (nonuterine) serous carcinomas of tubal origin? Am J Surg Pathol. 2010; 34:1407–16.
Article17. Kindelberger DW, Lee Y, Miron A, et al. Intraepithelial carcinoma of the fimbria and pelvic serous carcinoma: evidence for a causal relationship. Am J Surg Pathol. 2007; 31:161–9.
Article18. Tang S, Onuma K, Deb P, et al. Frequency of serous tubal intraepithelial carcinoma in various gynecologic malignancies: a study of 300 consecutive cases. Int J Gynecol Pathol. 2012; 31:103–10.19. Robey SS, Silva EG. Epithelial hyperplasia of the fallopian tube: its association with serous borderline tumors of the ovary. Int J Gynecol Pathol. 1989; 8:214–20.
Article20. Yanai-Inbar I, Siriaunkgul S, Silverberg SG. Mucosal epithelial proliferation of the fallopian tube: a particular association with ovarian serous tumor of low malignant potential? Int J Gynecol Pathol. 1995; 14:107–13.21. Clement PB. The pathology of endometriosis: a survey of the many faces of a common disease emphasizing diagnostic pitfalls and unusual and newly appreciated aspects. Adv Anat Pathol. 2007; 14:241–60.22. Modesitt SC, Tortolero-Luna G, Robinson JB, Gershenson DM, Wolf JK. Ovarian and extraovarian endometriosis-associated cancer. Obstet Gynecol. 2002; 100:788–95.
Article23. Quigley JC, Hart WR. Adenomatoid tumors of the uterus. Am J Clin Pathol. 1981; 76:627–35.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Microscopic lesions of fallopian tubes in endometrioid carcinoma of the endometrium: How effective are the macroscopic tubal sampling techniques?
- The electron microscopic changes of the mucosa of fallopian tubes after surgical sterilization
- A Case of Primary Carcinoma of the Fallopian Tube
- Three Case of Primary Carcinoma
- Primary Malignant Tumor of the Fallopian Tube: 2 cases Reports Papillary Carcinoma and Choriocarcionma
