A Systematic Classification of the Congenital Bronchopulmonary Vascular Malformations: Dysmorphogeneses of the Primitive Foregut System and the Primitive Aortic Arch System
- Affiliations
-
- 1Department of Pediatrics, Division of Pediatric Cardiology, Changhua Christian Hospital, Changhua, Taiwan. ferdielee@yahoo.com
- 2Department of Pediatrics, Division of Pediatric Cardiology, Min-Sheng General Hospital, Tao-Yuan, Taiwan.
- 3Department of Surgery, Division of Cardiovascular Surgery, College of Medicine, National Taiwan University Hospital, Taipei, Taiwan.
- 4Department of Pediatric Pulmonology, Changhua Christian Hospital, Changhua, Taiwan.
- 5Department of Pediatric Neonatology, Changhua Christian Hospital, Changhua, Taiwan.
- 6Department of Pediatric Surgery, Division of Chest Surgery, Changhua Christian Hospital, Changhua, Taiwan.
- 7Department of Radiology, Changhua Christian Hospital, Changhua, Taiwan.
Abstract
- PURPOSE
We reviewed the cases of 33 patients from our clinic and 142 patients from the literature with congenital bronchopulmonary vascular malformations (BPVM), systematically analyzed the bronchopulmonary airways, pulmonary arterial supplies, and pulmonary venous drainages, and classified these patients by pulmonary malinosculation (PM). MATERIALS AND METHODS: From January 1990 to January 2007, a total of 33 patients (17 men or boys and 16 women or girls), aged 1 day to 24 years (median, 2.5 months), with congenital BPVM were included in this study. Profiles of clinical manifestations, chest radiographs, echocardiographs, esophagographs, computer tomography (CT), magnetic resonance imaging (MRI), magnetic resonance angiography (MRA), cardiac catheterizations with angiography, contrast bronchographs, bronchoscopies, chromosomal studies, surgeries, and autopsies of these patients were analyzed to confirm the diagnosis of congenital BPVM. A total of 142 cases from the literature were also reviewed and classified similarly. RESULTS: The malformations of our 33 patients can be classified as type A isolated bronchial PM in 13 patients, type B isolated arterial PM in three, type C isolated venous PM in two, type D mixed bronchoarterial PM in five, type F mixed arteriovenous PM in one, and type G mixed bronchoarteriovenous PM in nine. CONCLUSION: Dysmorphogeneses of the primitive foregut system and the primitive aortic arch system may lead to haphazard malinosculations of the airways, arteries, and veins of the lung. A systematic classification of patients with congenital BPVM is clinically feasible by assessing the three basic bronchovascular systems of the lung independently.
Keyword
- Congenital bronchopulmonary vascular malformation; pulmonary malinosculation; scimitar syndrome; bronchopulmonary sequestration, sequestration spectrum, haphazard, dysmorphogeneses, primitive foregut system, primitive aortic ; sequestration spectrum, haphazard, dysmorphogeneses, primitive foregut system, primitive aortic arch system; haphazard, dysmorphogeneses, primitive foregut system, primitive aortic arch system; dysmorphogeneses, primitive foregut system, primitive aortic arch system; primitive foregut system, primitive aortic arch system; primitive aortic arch system
MeSH Terms
Figure
-
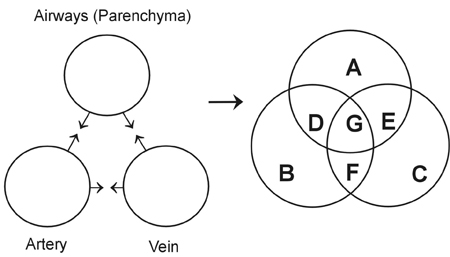
Fig. 1 Pulmonary malinosculation (PM) involving the pulmonary airways, the pulmonary artery, and the pulmonary vein independently. Each circle represents the occurrence of PM involving the pulmonary airways, the pulmonary artery, and the pulmonary vein within the lung parenchyma, respectively. Each single circle converges to intersect (denoted by 3 sets of reverse arrows) another two circles to form the geometric figure of a trefoil (as a mathematical Venn diagram), within which are seven exclusive areas (areas A-G) denoting seven distinct PM. Area A represents type A isolated bronchial PM (with normal pulmonary artery and veins). Area B represents type B isolated arterial PM (with normal pulmonary airways and veins). Area C represents type C isolated venous PM (with normal pulmonary airways and artery). Area D represents type D mixed bronchoarterial PM (with normal pulmonary veins). Area E represents type E mixed bronchovenous PM (with normal pulmonary artery). Area F represents type F mixed arteriovenous PM (with normal pulmonary airways). Area G represents type G mixed bronchoarteriovenous PM.
Reference
-
1. Clements BS, Warner JO. Pulmonary sequestration and related congenital bronchopulmonary-vascular malformations: nomenclature and classification based on anatomical and embryological considerations. Thorax. 1987. 42:401–408.
Article2. Clements BS, Warner JO, Shinebourne EA. Congenital bronchopulmonary vascular malformations: clinical application of a simple anatomical approach in 25 cases. Thorax. 1987. 42:409–416.
Article3. Lee ML, Tsao LY, Chaou WT, Yang AD, Yeh KT, Wang JK, et al. Revisit on congenital bronchopulmonary vascular malformations: a haphazard branching theory of malinosculations and its clinical classification and implication. Pediatr Pulmonol. 2002. 33:1–11.
Article4. Sade RM, Clouse M, Ellis FH Jr. The spectrum of pulmonary sequestration. Ann Thorac Surg. 1974. 18:644–658.
Article5. Panicek DM, Heitzman ER, Randall PA, Groskin SA, Chew FS, Lane EJ Jr, et al. The continuum of pulmonary developmental anomalies. Radiographics. 1987. 7:747–772.
Article6. Kirks DR, Kane PE, Free EA, Taybi H. Systemic arterial supply to normal basilar segments of the lower lobe. AJR Am J Roentgenol. 1976. 126:817–821.7. Blesovsky A. Pulmonary sequestration. A report of an unusual case and a review of the literature. Thorax. 1967. 22:351–357.8. Halasz NA, Halloran KH, Liebow AA. Bronchial and arterial anomalies with drainage of the right lung into the inferior vena cava. Circulation. 1956. 14:826–846.
Article9. Neill CA, Ferencz C, Sabiston DC, Sheldon H. The familial occurrence of hypoplastic right lung with systemic arterial supply and venous drainage "scimitar syndrome". Bull Johns Hopkins Hosp. 1960. 107:1–21.10. Reid L. 1976 Edward B.D. Neuhauser lecture: the lung: growth and remodeling in health and disease. AJR Am J Roentgenol. 1977. 129:777–788.
Article11. Congdon ED. Transformation of the aortic arch system during the development of the human embryo. Contrib Embryol. 1922. 14:47–110.12. Huntington GS. The morphology of the pulmonary artery in the mammalia. Anat Rec. 1919. 17:165–190.
Article13. Cucci CE, Doyle EF, Lewis EW Jr. Absence of a primary division of the pulmonary trunk. An ontogenetic theory. Circulation. 1964. 29:124–131.
Article14. Neill CA. Development of the pulmonary veins; with reference to the embryology of anomalies of pulmonary venous return. Pediatrics. 1956. 18:880–887.15. Lee ML, Yang SC, Yang AD. Transcatheter occlusion of the isolated scimitar vein anomaly camouflaged under dual pulmonary venous drainage of the right lung by the Amplatzer Ductal Occluder. Int J Cardiol. 2007. 115:e90–e93.
Article16. Juraszek AL, Cohn H, van Praagh R, van Praagh S. Isolated left-sided scimitar vein connecting all left pulmonary veins to the right inferior vena cava. Pediatr Cardiol. 2005. 26:846–847.17. Phoon CK, Neill CA. Asplenia syndrome: insight into embryology through an analysis of cardiac and extracardiac anomalies. Am J Cardiol. 1994. 73:581–587.
Article18. Sissman NJ. Developmental landmarks in cardiac morphogenesis: comparative chronology. Am J Cardiol. 1970. 25:141–148.
Article19. Boyden EA. The time lag in the development of bronchial arteries. Anat Rec. 1970. 166:611–614.
Article20. Rabinovitch M, Herrera-deLeon V, Castaneda AR, Reid L. Growth and development of the pulmonary vascular bed in patients with tetralogy of Fallot with or without pulmonary atresia. Circulation. 1981. 64:1234–1249.
Article21. Zaw-Tun HA. The tracheo-esophageal septum-fact or fantasy? Origin and development of the respiratory primordium and esophagus. Acta Anat (Basel). 1982. 114:1–21.22. Gerle RD, Jaretzki A 3rd, Ashley CA, Berne AS. Congenital bronchopulmonary-foregut malformation. Pulmonary sequestration communicating with the gastrointestinal tract. N Engl J Med. 1968. 278:1413–1419.23. Felker RE, Tonkin IL. Imaging of pulmonary sequestration. AJR Am J Roentgenol. 1990. 154:241–249.
Article24. Smith RA. A theory of the origin of intralobar sequestration of lung. Thorax. 1956. 11:10–24.
Article25. Boyden EA. Bronchogenic cysts and the theory of intralobar sequestration: new embryologic data. J Thorac Surg. 1958. 35:604–616.
Article26. Pryce DM. Lower accessory pulmonary artery with intralobar sequestration of lung: a report of seven cases. J Pathol Bacteriol. 1946. 58:457–467.
Article27. Thilenius OG, Ruschhaupt DG, Replogle RL, Bharati S, Herman T, Arcilla RA. Spectrum of pulmonary sequestration: association with anomalous pulmonary venous drainage in infants. Pediatr Cardiol. 1983. 4:97–103.
Article28. Flisak ME, Chandrasekar AJ, Marsan RE, Ali MM. Systemic arterialization of lung without sequestration. AJR Am J Roentgenol. 1982. 138:751–753.
Article29. Cooper G. Case of malformation of the thoracic viscera: Consisting of imperfect development of right lung and transposition of the heart. London Med Gazzette. 1836. 18:600–601.30. Chassinat R. Observation d'anomalies anatomiques remarquables de l'appareil circulatoire, avec hepatocele congeniale, n'ayant donne lieu pendant la vie a aucun symptom particulier. Arch Genet Med. 1836. 11:80–84.31. Morgan JR, Forker AD. Syndrome of hypoplasia of the right lung and dextroposition of the heart: "scimitar sign" with normal pulmonary venous drainage. Circulation. 1971. 43:27–30.
Article32. Kanemoto N, Sugiyama T, Hirose S, Goto Y. A case with pseudo-scimitar syndrome: "scimitar sign" with normal pulmonary venous drainage. Jpn Circ J. 1987. 51:642–646.
Article33. Herer B, Jaubert F, Delaisements C, Huchon G, Chretien J. Scimitar sign with normal pulmonary venous drainage and anomalous inferior vena cava. Thorax. 1988. 43:651–652.
Article34. Cukier A, Kavakama J, Teixeira LR, Terra-Filho M, Vargas FS. Scimitar sign with normal pulmonary venous drainage and systemic arterial supply. Scimitar syndrome or bronchopulmonary sequestration? Chest. 1994. 105:294–295.
Article35. Gikonyo DK, Tandon R, Lucas RV Jr, Edwards JE. Scimitar syndrome in neonates: a report of four cases and review of the literature. Pediatr Cardiol. 1986. 6:193–197.
Article36. Partridge JB, Osborne JM, Slaughter RE. Scimitar etcetera-the dysmorphic right lung. Clin Radiol. 1988. 39:11–19.37. Dupuis C, Charaf LA, Brevière GM, Abou P, Rémy-Jardin M, Helmius G. The "adult" form of the scimitar syndrome. Am J Cardiol. 1992. 70:502–507.
Article38. Dupuis C, Charaf LA, Brevière GM, Abou P. "Infantile" form of the scimitar syndrome with pulmonary hypertension. Am J Cardiol. 1993. 71:1326–1330.
Article39. Pearl W. Scimitar variant. Pediatr Cardiol. 1987. 8:139–141.
Article40. Tumbarello R, Abbruzzese PA, Meloni G, Porcu M, Martelli V, Sanna A. A variant of the scimitar syndrome with stenosed drainage of the inferior vena cava. Am Heart J. 1991. 121:616–618.
Article41. Oakley D, Naik D, Verel D, Rajan S. Scimitar vein syndrome: report of nine new cases. Am Heart J. 1984. 107:596–598.
Article42. Rose C, Vosshenrich R. Incomplete scimitar syndrome. Cardiol Young. 2002. 12:389–390.
Article43. Freedom RM, Burrows PE, Moes CA. "Horseshoe" lung: report of five new cases. AJR Am J Roentgenol. 1986. 146:211–215.
Article44. Frank JL, Poole CA, Rosas G. Horseshoe lung: clinical, pathologic, and radiologic features and a new plain film finding. AJR Am J Roentgenol. 1986. 146:217–226.
Article45. Dupuis C, Rémy J, Rémy-Jardin M, Coulomb M, Brevière GM, Ben Laden S. The "horseshoe" lung: six new cases. Pediatr Pulmonol. 1994. 17:124–130.
Article46. Clements BS, Warner JO. The crossover lung segment: congenital malformation associated with a variant of scimitar syndrome. Thorax. 1987. 42:417–419.
Article47. Gikonyo BM, Jue KL, Edwards JE. Pulmonary vascular sling: report of seven cases and review of the literature. Pediatr Cardiol. 1989. 10:81–89.
Article48. Bamman JL, Ward BH, Woodrum DE. Aberrant left pulmonary artery. Clinical and embryologic factors. Chest. 1977. 72:67–71.49. Wells TR, Gwinn JL, Landing BH, Stanley P. Reconsideration of the anatomy of sling left pulmonary artery: the association of one form with bridging bronchus and imperforate anus. Anatomic and diagnostic aspects. J Pediatr Surg. 1988. 23:892–898.
Article50. Frischer T, Holomanova I, Frenzel K, Wollenek G, Wimmer M. Therapeutic strategy in a 9-month-old child with pulmonary sling: need for bronchoscopic evaluation. Pediatr Cardiol. 1996. 17:201–203.
Article51. Boothroyd AE, Carty H, Arnold R. Shoe, scimitar or sequestration: a shifting spectrum. Pediatr Radiol. 1995. 25:652–653.
Article52. Woodring JH, Howard TA, Kanga JF. Congenital pulmonary venolobar syndrome revisited. Radiographics. 1994. 14:349–369.
Article53. Gao YA, Burrows PE, Benson LN, Rabinovitch M, Freedom RM. Scimitar syndrome in infancy. J Am Coll Cardiol. 1993. 22:873–882.
Article54. Geggel RL. Scimitar syndrome associated with partial anomalous pulmonary venous connection at the supracardiac, cardiac, and infracardiac levels. Pediatr Cardiol. 1993. 14:234–237.
Article55. Dickinson DF, Galloway RW, Massey R, Sankey R, Arnold R. Scimitar syndrome in infancy. Role of embolization of systemic arterial supply to right lung. Br Heart J. 1982. 47:468–472.
Article56. Farnsworth AE, Ankeney JL. The spectrum of the scimitar syndrome. J Thorac Cardiovasc Surg. 1974. 68:37–42.
Article57. Schramel FM, Westermann CJ, Knaepen PJ, van den Bosch JM. The scimitar syndrome: clinical spectrum and surgical treatment. Eur Respir J. 1995. 8:196–201.
Article58. Rutledge JM, Hiatt PW, Wesley Vick G 3rd, Grifka RG. A sword for the left hand: an unusual case of left-sided scimitar syndrome. Pediatr Cardiol. 2001. 22:350–352.
Article59. Le Rochais JP, Icard P, Davani S, Abouz D, Evrard C. Scimitar syndrome with pulmonary arteriovenous fistulas. Ann Thorac Surg. 1999. 68:1416–1418.
Article60. Beitzke A, Zobel G, Rigler B, Stein JI, Suppan C. Scimitar syndrome with absence of the right pulmonary artery: a case with volume-induced, reversible, left-sided pulmonary hypertension. Pediatr Cardiol. 1992. 13:119–121.
Article61. Heron CW, Pozniak AL, Hunter GJ, Johnson NM. Anomalous systemic venous drainage occurring in association with the hypogenetic lung syndrome. Clin Radiol. 1988. 39:446–449.
Article62. Tummers RF, Lam J, Nijveld A, Marcelletti C, Losekoot G. An infant with the scimitar syndrome and pulmonary hypertension; successful surgical intervention. Eur Heart J. 1987. 8:194–197.
Article63. Honey M. Anomalous pulmonary venous drainage of right lung to inferior vena cava ('scimitar syndrome'): clinical spectrum in older patients and role of surgery. Q J Med. 1977. 184:463–483.64. Folger GM. The scimitar syndrome. Anatomic, physiologic, developmental and therapeutic considerations. Angiology. 1976. 27:373–407.
Article65. Jue KL, Amplatz K, Adams P Jr, Anderson RC. Anomalies of great vessels associated with lung hypoplasia. The scimitar syndrome. Am J Dis Child. 1966. 111:35–44.
Article66. Macpherson RI, Whytehead L. Pseudosequestration. J Can Assoc Radiol. 1977. 28:17–25.67. Alivizatos P, Cheatle T, de Leval M, Stark J. Pulmonary sequestration complicated by anomalies of pulmonary venous return. J Pediatr Surg. 1985. 20:76–79.
Article68. Orzan F, Angelini P, Oglietti J, Leachman RD, Cooley DA. Horses lung: Report of two cases. Am Heart J. 1977. 93:501–505.69. Telander RL, Lennox C, Sieber W. Sequestration of the lung in children. Mayo Clin Proc. 1976. 51:578–584.70. Weisel W, Docksey JW, Glicklich M. Vascular anomalies associated with intrapulmonary bronchial cysts. Am Rev Tuberc. 1955. 71:573–583.71. Currarino G, Willis K, Miller W. Congenital fistula between an aberrant systemic artery and a pulmonary vein without sequestrations. A report of three cases. J Pediatr. 1975. 87:554–557.
Article72. Jona JZ, Raffensperger JG. Total sequestration of the lung. J Thorac Cardiovasc Surg. 1975. 69:361–364.73. Kafka V, Beco V. Simultaneous intra- and extrapulmonary sequestration. Arch Dis Child. 1960. 35:51–56.
Article74. Roe JP, Mack JW, Shirley JH. Bilateral pulmonary sequestrations. J Thorac Cardiovasc Surg. 1980. 80:8–10.
Article75. Lacina S, Townley R, Radecki L, Stockinger F, Wyngaarden M. Esophageal lung with cardiac abnormalities. Chest. 1981. 79:468–470.
Article76. Fusonie D, Molnar W. Anomalous pulmonary venous return, pulmonary sequestration, bronchial atresia, aplastic right upper lobe, pericardial defect and intrathoracic kidney. An unusual complex of congenital anomlies in one patient. Am J Roentgenol Radium Ther Nucl Med. 1966. 97:350–354.
Article77. Heithoff KB, Sane SM, Williams HJ, Jarvis CJ, Carter J, Kane P, et al. Bronchopulmonary foregut malformations. A unifying etiological concept. AJR Am J Roentgenol. 1976. 126:46–55.
Article78. Cipriano P, Sweeney LJ, Hutchins GM, Rosenquist GC. Horseshoe lung in an infant with recurrent pulmonary infections. Am J Dis Child. 1975. 129:1343–1345.
Article79. Moerman P, Vandenberghe K, Devlieger H, Van Hole C, Fryns JP, Lauweryns JM. Congenital pulmonary lymphangiectasis with chylothorax: a heterogeneous lymphatic vessel abnormality. Am J Med Genet. 1993. 47:54–58.
Article80. Gazzaniga AB, Matloff JM, Harken DE. Anomalous right pulmonary venous drainage into the inferior vena cava and left atrium. J Thorac Cardiovasc Surg. 1969. 57:251–254.
Article81. Tortoriello TA, Vick GW 3rd, Chung T, Bezold LI, Vincent JA. Meandering right pulmonary vein to the left atrium and inferior vena cava: the first case with associated anomalies. Tex Heart Inst J. 2002. 29:319–323.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Congenital Bronchopulmonary Foregut Malformation: Analysis of the surgical and autopsy cases
- Primitive Neuroectodermal Tumor of the Kidney with CD99 Positive Staining
- A case of primitive persistent hypoglossal artery
- A Communicating Bronchopulmonary Foregut Malformation Associated with Absence of the Left Pericardium: A case report
- Persistent Primitive Trigeminal Artery That Mimics Persistent Primitive Otic Artery on Cerebral Angiography
