Astigmatic Analysis before and after Surgical Excision of Limbal Dermoid: Functional Outcome
- Affiliations
-
- 1Department of Ophthalmology, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. vaccine@catholic.ac.kr
- KMID: 2390074
- DOI: http://doi.org/10.3341/jkos.2017.58.9.1092
Abstract
- PURPOSE
To analyze the length and area of limbal dermoid invading the cornea and to evaluate the effects on visual acuity and astigmatism before and after surgery.
METHODS
This retrospective study included 20 eyes of 20 patients who underwent surgical removal of limbal dermoid. The preoperative and postoperative visual acuity and astigmatism level were measured. In addition, we evaluated the correlations of astigmatism with the length ratio (length of limbal dermoid invading the cornea/total corneal diameter), width ratio (width of limbal dermoid invading the cornea/total corneal diameter), and area ratio (area of limbal dermoid invading the cornea/total corneal area) using preoperative anterior segment photographs.
RESULTS
The mean preoperative astigmatism was 0.85 ± 0.71 D in the sound eye and 3.00 ± 3.14 D in the affected eye (p = 0.004). Length, width, and area ratio of limbal dermoid have positive correlation with astigmatism (p < 0.010 for all variables), with a larger length ratio of limbal dermoid invading the cornea producing greater reduction in postoperative astigmatism (p = 0.010, r = 0.816). The amount of astigmatism was significantly higher in patients with amblyopia in the affected eye (p = 0.030). Visual acuity gain more than 2 lines was achieved in 8 among 10 patients with amblyopia under the age of 7 years through the appropriate refractive correction and occlusion 1 year after surgery.
CONCLUSIONS
Astigmatism is a major cause of amblyopia in pediatric patients with limbal dermoid. The degree of astigmatism can be predicted by the size factors of the limbal dermoid. In particular, the relative length of limbal dermoid invading the cornea has a stronger correlation with preoperative astigmatism than other factors and has correlation with postoperative reduction of astigmatism. It should be emphasized that children with limbal dermoid need appropriate refractive correction and occlusion in addition to surgical excision.
Keyword
Figure
-
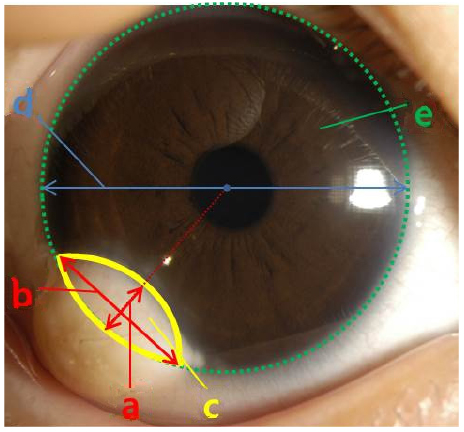
Figure 1 The parameter of limbal dermoid size by graphic program. (a) is limbal dermoid horizontal length to corneal center. (b) is distance between 2 limbal points where the limbal dermoid intersected with the limbus. (c) is area of limbal dermoid on cornea. (d) is total corneal diameter. (e) is total corneal area. Relative length is (a)/(d), relative width is (b)/(d), and relative area is (c)/(e).

Figure 2 The preoperative astigmatism and the change of astigmatism according to the length of the central invasion of the limbal dermoid. The corneal diameter is assumed to be 11.5 mm. (A) Scatterplot graph showing a positive linear correlation between limbal dermoid length invading cornea (in millimeters) and preoperative astigmatism (in diopters). (B) Scatterplot graph showing a positive linear correlation between limbal dermoid length invading cornea (in millimeters) and variation between preoperative and postoperative astigmatism. Pre op. = preoperative; D = diopter.
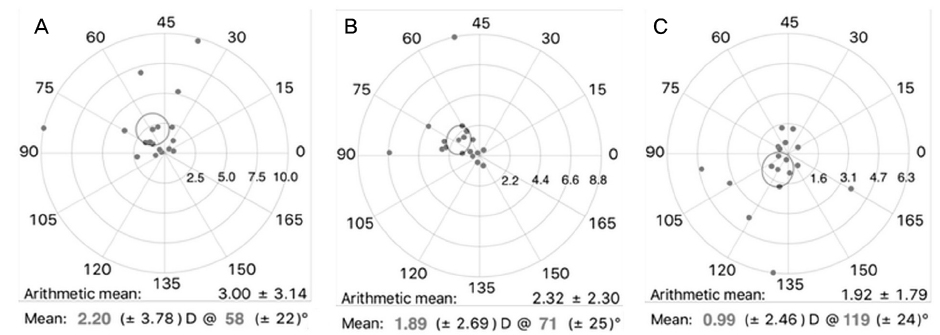
Figure 3 Double-angle scatterplots of astigmatism using AstigPLOT. Only 17 eyes with the center of the limbal dermoid located on the inferotemporal side were included. (A) Scatter plot of polar astigmatic vectors for preoperative astigmatism (n = 17). (B) Scatter plot of polar astigmatic vectors for postoperative astigmatism (n = 17). (C) Scatter plot of calculated surgically induced astigmatism (n = 17). Astigmatism was expressed on a negative scale. Blue one point represents one eye and red point represents centroid. The distance from the origin to a point represents the size of the induced corneal astigmatism, and each graph has a single size displayed. D = diopter.
Reference
-
1. Mansour AM, Barber JC, Reinecke RD, Wang FM. Ocular choristomas. Surv Ophthalmol. 1989; 33:339–358.2. Elsas FJ, Green WR. Epibulbar tumors in childhood. Am J Ophthalmol. 1975; 79:1001–1007.3. Cunha RP, Cunha MC, Shields JA. Epibulbar tumors in children: a survey of 282 biopsies. J Pediatr Ophthalmol Strabismus. 1987; 24:249–254.4. Robb RM. Astigmatic refractive errors associated with limbal dermoids. J Pediatr Ophthalmol Strabismus. 1996; 33:241–243.5. Nevares RL, Mulliken JB, Robb RM. Ocular dermoids. Plast Reconstr Surg. 1988; 82:959–964.6. Benjamin SN, Allen HF. Classification for limbal dermoid choristomas and branchial arch anomalies. Presentation of an unusual case. Arch Ophthalmol. 1972; 87:305–314.7. Pirouzian A. Management of pediatric corneal limbal dermoids. Clin Ophthalmol. 2013; 7:607–614.8. Grossniklaus HE, Green WR, Luckenbach M, Chan CC. Conjunctival lesions in adults. A clinical and histopathologic review. Cornea. 1987; 6:78–116.9. Kodsi SR, Bloom KE, Egbert JE, et al. Ocular and systemic manifestations of encephalocraniocutaneous lipomatosis. Am J Ophthalmol. 1994; 118:77–82.10. Scott JA, Tan DT. Therapeutic lamellar keratoplasty for limbal dermoids. Ophthalmology. 2001; 108:1858–1867.11. Mansour AM, Wang F, Henkind P, et al. Ocular findings in the facioauriculovertebral sequence (Goldenhar-Gorlin syndrome). Am J Ophthalmol. 1985; 100:555–559.12. Wick B, Wingard M, Cotter S, Scheiman M. Anisometropic amblyopia: is the patient ever too old to treat? Optom Vis Sci. 1992; 69:866–878.13. Kim SA, Jung SK, Paik JS, Yang SW. Effect of orbital decompression on corneal topography in patients with thyroid ophthalmopathy. PLoS One. 2015; 10:e0133612.14. Yoon CK, Kim JH, Kim SJ, Yu YS. The surgical outcomes of simple keratectomy for limbal dermoids. J Korean Ophthalmol Soc. 2008; 49:897–903.15. Donahue SP, Arnold RW, Ruben JB. AAPOS Vision Screening Committee. Preschool vision screening: what should we be detecting and how should we report it? Uniform guidelines for reporting results of preschool vision screening studies. J AAPOS. 2003; 7:314–316.16. Panton RW, Sugar J. Excision of limbal dermoids. Ophthalmic Surg. 1991; 22:85–89.17. Shen YD, Chen WL, Wang IJ, et al. Full-thickness central corneal grafts in lamellar keratoscleroplasty to treat limbal dermoids. Ophthalmology. 2005; 112:1955.18. Panda A, Ghose S, Khokhar S, Das H. Surgical outcomes of Epibulbar dermoids. J Pediatr Ophthalmol Strabismus. 2002; 39:20–25.19. Holladay JT, Dudeja DR, Koch DD. Evaluating and reporting astigmatism for individual and aggregate data. J Cataract Refract Surg. 1998; 24:57–65.20. Borasio E, Mehta JS, Maurino V. Surgically induced astigmatism after phacoemulsification in eyes with mild to moderate corneal astigmatism: temporal versus on-axis clear corneal incisions. J Cataract Refract Surg. 2006; 32:565–572.
