A Congenital Gerbode Defect associated with a Rare Structural Abnormality of the Mitral Valve Diagnosed in an Adult Patient
- Affiliations
-
- 1University of Medicine and Pharmacy, Carol Davila, Romania. euroecolab@gmail.com
- 2Department of Cardiology, Emergency Institute of Cardiovascular Diseases, Bucharest, Romania.
- KMID: 2389635
- DOI: http://doi.org/10.4070/kcj.2016.46.5.739
Abstract
- We report the case of a rare association of a congenital Gerbode defect with severe mitral regurgitation due to abnormal linear structure of mitral valve, diagnosed in an adult patient. The case highlights the importance of a thorough examination interpreting the echocardiographic findings on a pathophysiological basis. It also underlines the complementary role of different imaging techniques with transesophageal echocardiography, allowing the precise assessment of both structural and functional abnormalities in such a complex case. The patient underwent mitral valve replacement with a bileaflet mechanical prosthesis and repair of the Gerbode defect. The imaging findings were confirmed during the surgical procedure, leading to a good outcome.
Keyword
MeSH Terms
Figure
-
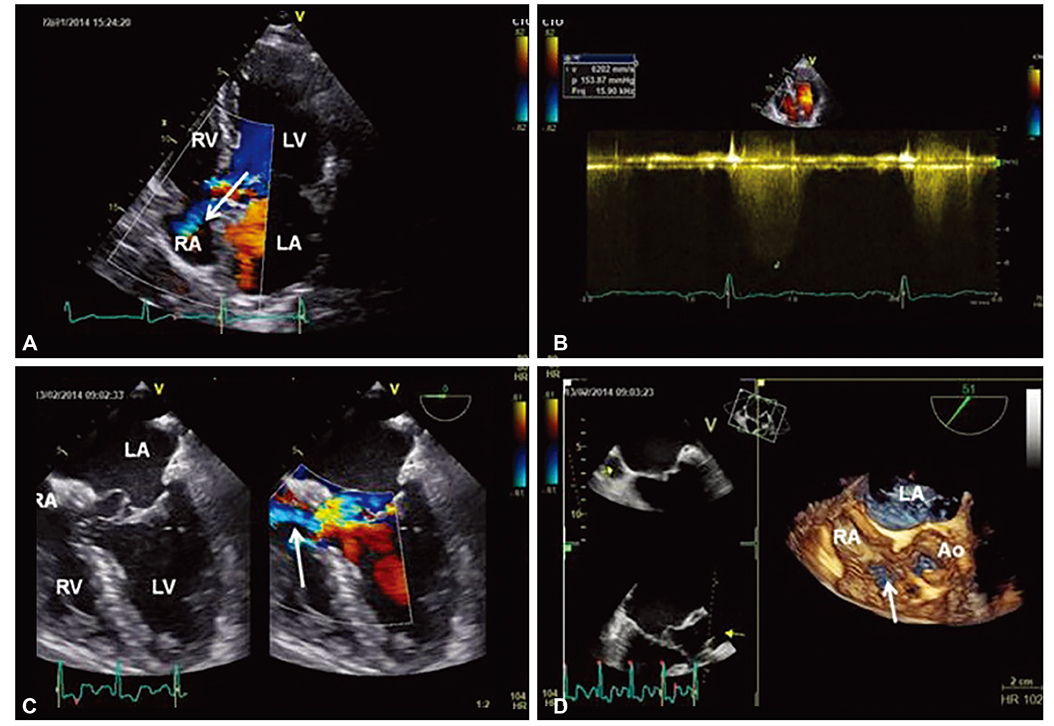
Fig. 1 Echocardiographic imagings. (A) Transthoracic echocardiography, apical 4-chamber view. High velocity jet from a small Gerbode type defect (white arrow). (B) CW-Doppler revealing a high velocity systolic jet (maximum velocity of 5.2 m/s) simulating severe pulmonary arterial hypertension. (C) Transesophageal echocardiography (0°), mid-esophageal 4-chamber view. Intracardiac shunt (white arrow) toward the RA from the LV in midsystole. (D) 3D Transesophageal echocardiography confirms the communication between the LV and the RA consistent with a Gerbode defect (white arrow). RV: right ventricle, LV: left ventricle, RA: right atrium, LA: left atrium. CW: continuous wave.
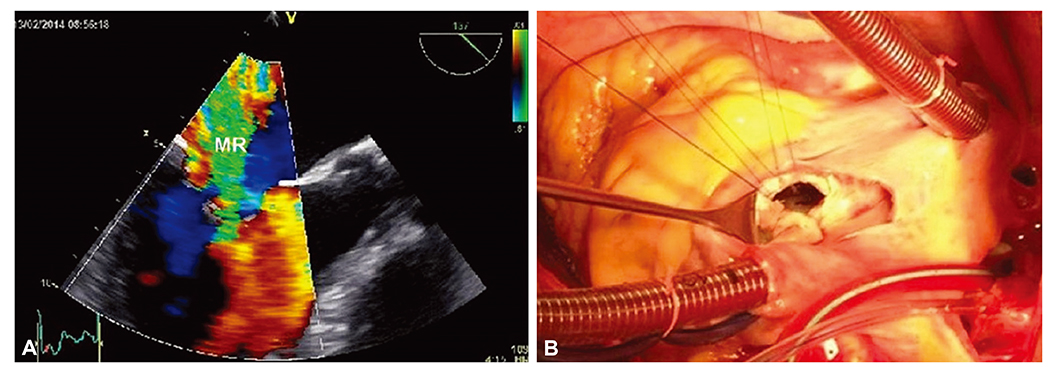
Fig. 2 (A) Transesophageal echocardiography, Color Doppler mid-esophageal long-axis view shows severe mitral regurgitation (Vena Contracta 7 mm). (B) The intraoperative view confirms the LV to RA communication. LV: left ventricle, RA: right atrium, MR: mitral regurgitation.
Reference
-
1. Laurichesse J, Ferrane J, Renais J, Scebat L, Lenegre J. Communication between the left ventricle and the right auricle. Arch Mal Coeur Vaiss. 1964; 57:703–724.2. Thurnan J. On aneurisms of the heart with cases. Med Chir Trans. 1838; 21:187–438.3. Gerbode F, Hultgren H, Melrose D, Osborn J. Syndrome of left ventricular–right atrial shunt: successful surgical repair of defect in five cases, with observation of bradycardia on closure. Ann Surg. 1958; 148:433–446.4. Kelle AM, Young L, Kaushal S, Duffy CE, Anderson RH, Backer CL. The Gerbode defect: the significance of a left ventricular to right atrial shunt. Cardiol Young. 2009; 19:Suppl 2. 96–99.5. Acar P, Séguela PE, Hascoet S. The Gerbode defect or left ventricular to right atrial shunt assessed by transthoracic 3D echocardiography. Echocardiography. 2011; 28:E140–E142.6. Hansalia S, Manda J, Pothineni KR, Nanda NC. Usefulness of live/real time three-dimensional transthoracic echocardiography in diagnosing acquired left ventricular–right atrial communication misdiagnosed as severe pulmonary hypertension by two-dimensional transthoracic echocardiography. Echocardiography. 2009; 26:224–227.7. Tehrani F, Movahed MR. How to prevent echocardiographic misinterpretation of Gerbode type defect as pulmonary arterial hypertension. Eur J Echocardiogr. 2007; 8:494–497.8. Taskesen T, Prouse AF, Goldberg SL, Gill EA. Gerbode defect: another nail for the 3D transesophageal echo hammer? Int J Cardiovasc Imaging. 2015; 31:753–764.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Isolated Congenital Double-Orifice Mitral Valve
- A Case of Turner's Syndrome Associated with Atrial Septal Defect and Mitral Valve Prolapse
- Real Time Three-Dimensional Echocardiographic Detection of Acquried Left Ventricular-Right Atrial Communication (Gerbode-Type Defect) Caused by Infectious Endocarditis
- A Case of Parachute Mitral Valve in an Adult
- Rare Case of Unileaflet Mitral Valve
