Contralateral Nerve Root Compression after Direct Lateral Lumbar Interbody Fusion
- Affiliations
-
- 1Department of Orthopaedic Surgery, Pusan National University School of Medicine, Busan, Korea. jungsublee@pusan.ac.kr
- KMID: 2384560
- DOI: http://doi.org/10.4055/jkoa.2017.52.3.285
Abstract
- Direct lateral lumbar interbody fusion (DLIF) has been introduced as an effective new thoracolumbar fusion technique for patients with degenerative lumbar diseases. DLIF associated with easy-to-learn, high fusion rate, improved restoration of spinal alignment, and early patient mobilization due to minimally invasive nature. However, ipsilateral L2-L5 nerve root irritation and injury are well-known complications. However, damage to the contralateral nerve root has been rarely reported and, to the best of our knowledge, there have not been any reports about contralateral nerve root injury after DLIF in Korea. Thus, we report a case of contralateral nerve root compression due to osteophyte from the lower endplate of the vertebral body and position of intervertebral cage after DLIF.
MeSH Terms
Figure
-
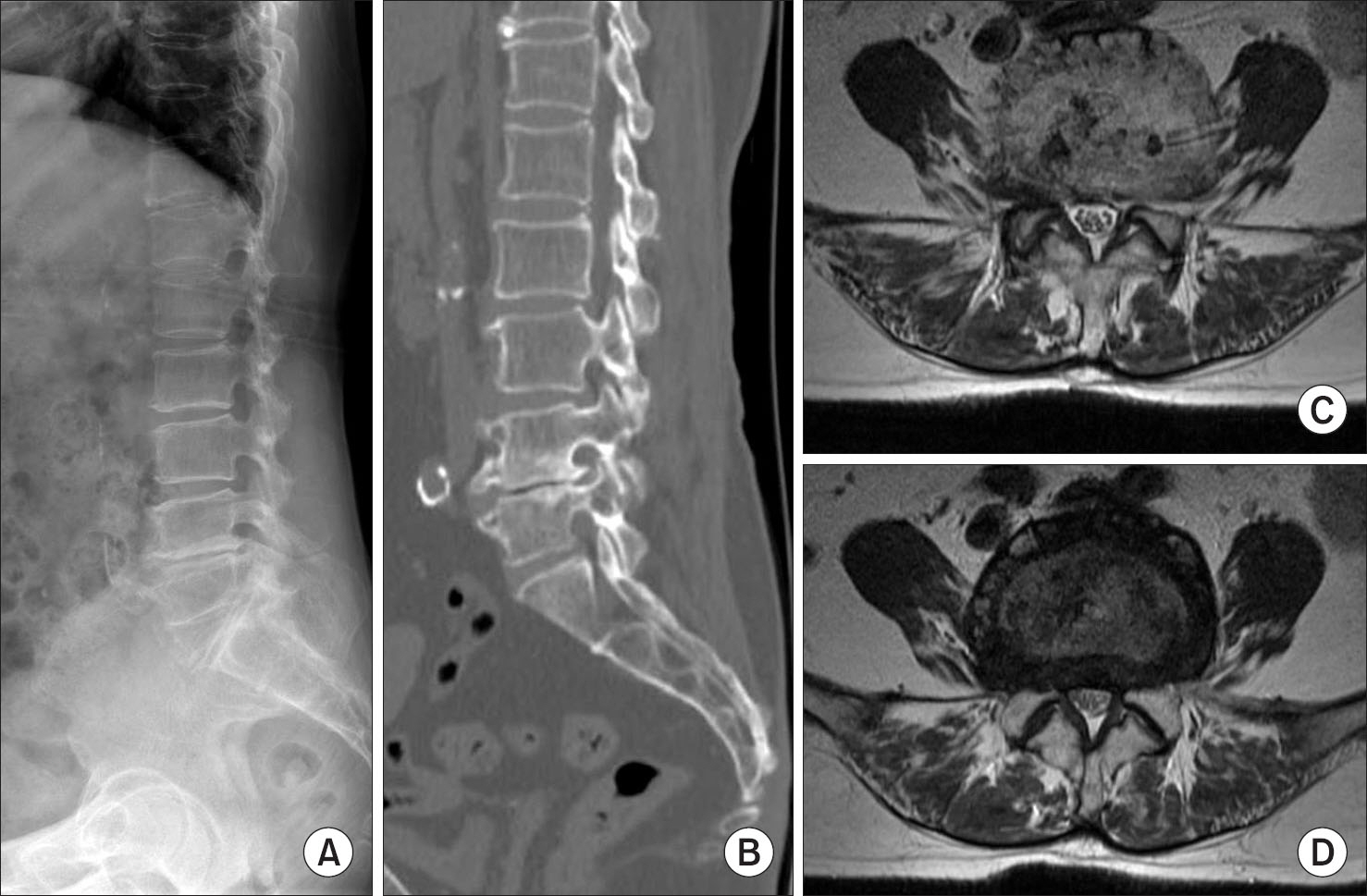
Figure 1 A 72-year-old female patient with L4–5 spinal stenosis. (A) Loss of lumbar lordosis and L4–5 severe degenerative change is shown on lateral radiography. (B) Enlarged osteophytes are shown around L4–5 and right L4 foraminal space. (C, D) Severe central and foraminal spinal stenosis at the L4–5 level in T2-weighted magnetic resonance imagings, especially with greater severity on the right side.

Figure 2 Postoperative radiographs. Anteroposterior (A) and lateral (B) radiographs show direct lateral lumbar interbody fusion, posterior decompression and fusion using pedicle screws on L4–5 level. On lateral radiograph, enlarged intervertebral and foraminal spaces are shown.
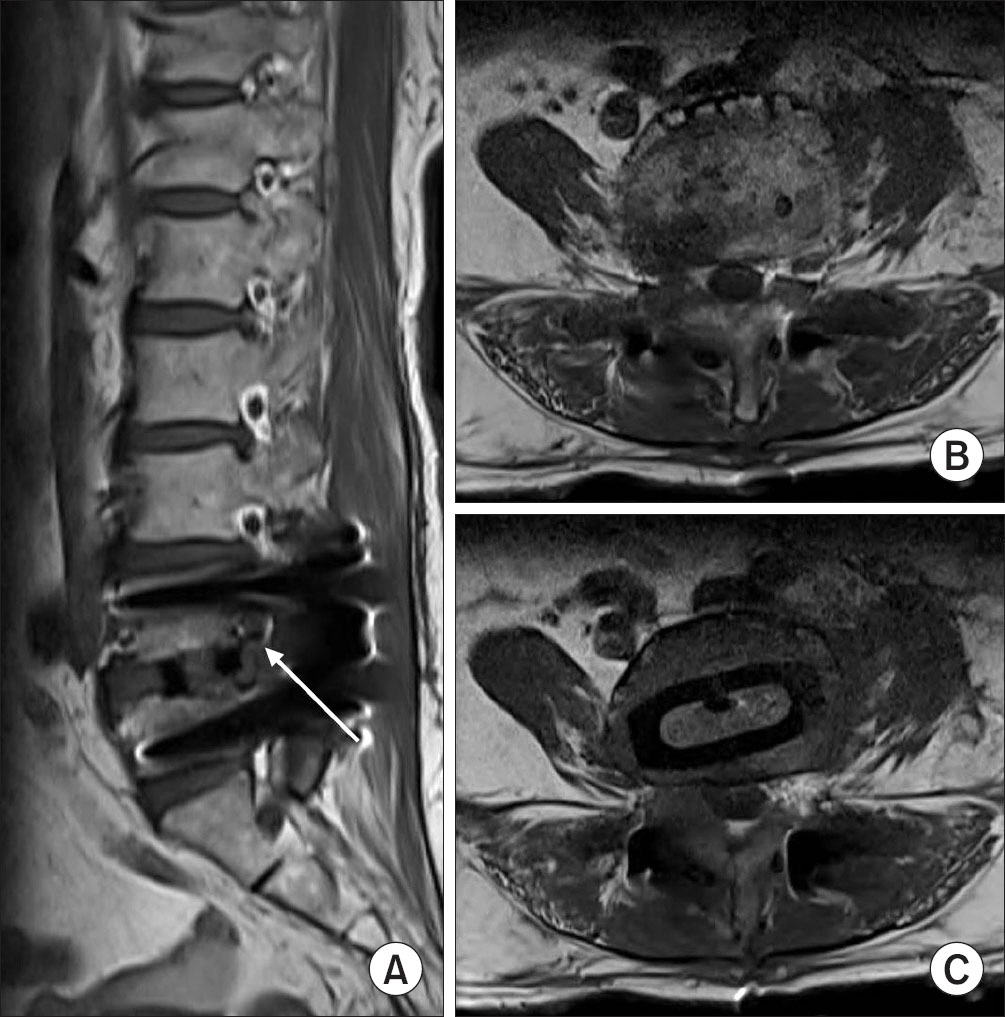
Figure 3 Postoperative T1-weighted magnetic resonance imagings. Right L4–5 neural foramen is severe narrowed (A, white arrow) and L4 nerve root is compressed even though after surgery (B). (C) Interbody cage is located diagonally with direction from left anterior entry point to right posterior near right neural foramen.
Reference
-
1. McAfee PC, Regan JJ, Geis WP, Fedder IL. Minimally invasive anterior retroperitoneal approach to the lumbar spine. Emphasis on the lateral BAK. Spine (Phila Pa 1976). 1998; 23:1476–84.2. Ozgur BM, Aryan HE, Pimenta L, Taylor WR. Extreme lateral interbody fusion (XLIF): a novel surgical technique for anterior lumbar interbody fusion. Spine J. 2006; 6:435–43.
Article3. Oliveira L, Marchi L, Coutinho E, Pimenta L. A radiographic assessment of the ability of the extreme lateral interbody fusion procedure to indirectly decompress the neural elements. Spine (Phila Pa 1976). 2010; 35:S331–7.
Article4. Sharma AK, Kepler CK, Girardi FP, Cammisa FP, Huang RC, Sama AA. Lateral lumbar interbody fusion: clinical and radiographic outcomes at 1 year: a preliminary report. J Spinal Disord Tech. 2011; 24:242–50.5. Rodgers WB, Gerber EJ, Patterson J. Intraoperative and early postoperative complications in extreme lateral interbody fusion: an analysis of 600 cases. Spine (Phila Pa 1976). 2011; 36:26–32.6. Cappuccino A, Cornwall GB, Turner AW. . Biomechanical analysis and review of lateral lumbar fusion constructs. Spine (Phila Pa 1976). 2010; 35:S361–7.
Article7. Kepler CK, Sharma AK, Huang RC. . Indirect foraminal decompression after lateral transpsoas interbody fusion. J Neurosurg Spine. 2012; 16:329–33.
Article8. Houten JK, Alexandre LC, Nasser R, Wollowick AL. Nerve injury during the transpsoas approach for lumbar fusion. J Neurosurg Spine. 2011; 15:280–4.
Article9. Lykissas MG, Aichmair A, Hughes AP. . Nerve injury after lateral lumbar interbody fusion: a review of 919 treated levels with identification of risk factors. Spine J. 2014; 14:749–58.
Article10. Papanastassiou ID, Eleraky M, Vrionis FD. Contralateral femoral nerve compression: an unrecognized complication after extreme lateral interbody fusion (XLIF). J Clin Neurosci. 2011; 18:149–51.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Minimally Invasive Lateral Lumbar Interbody Fusion: Indications, Outcomes and Complications
- Uniportal Endoscopic Lumbar Interbody Fusion
- Pearls and Pitfalls of Oblique Lateral Interbody Fusion: A Comprehensive Narrative Review
- Minimally Invasive Lateral Lumbar Interbody Fusion: Surgical Technique and Review
- Morphometric Analysis of the Ureter with Respect to Lateral Lumbar Interbody Fusion Using Contrast-Enhanced Computed Tomography
