Mediastinal Pancreatic Pseudocysts
- Affiliations
-
- 1Department of Gastroenterology, Pomeranian Medical University, Szczecin, Poland. dabkowskikrzysztof@wp.pl
- 2Department of Thoracic Surgery and Transplantation, Pomeranian Medical University, Szczecin, Poland.
- 3Department of Radiology, Pomeranian Medical University, Szczecin, Poland.
- KMID: 2383494
- DOI: http://doi.org/10.5946/ce.2016.089
Abstract
- Mediastinal pseudocysts are a rare complication of acute pancreatitis. Lack of uniform treatment standards makes the management of this condition a clinical challenge. We report the case of a 43-year-old patient who presented with a left pleural effusion. Pleural fluid revealed a high amylase concentration consistent with a pancreaticopleural fistula. Endoscopic retrograde cholangiopancreatography (ERCP) revealed a disruption of the pancreatic duct with free outflow of contrast medium into the thoracic cavity. A pancreatic stent was placed. The second day after the ERCP, the patient developed septic shock and was admitted to the intensive care unit. Computed tomography (CT) revealed mediastinal pseudocysts and bilateral pleural effusions. After bilateral drainage of the pleural cavities, the patient improved clinically, and a follow-up CT scan showed that the fluid collection and pseudocysts had resolved. We discuss the optimal strategies for diagnosing and treating patients with pancreatic thoracic pseudocysts and fistulas, as well as review the management of these conditions.
Keyword
MeSH Terms
Figure
-
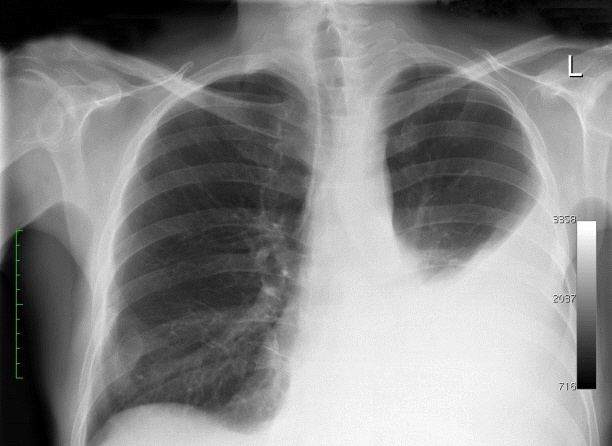
Fig. 1. Chest radiograph demonstrating fluid in the left pleural cavity.
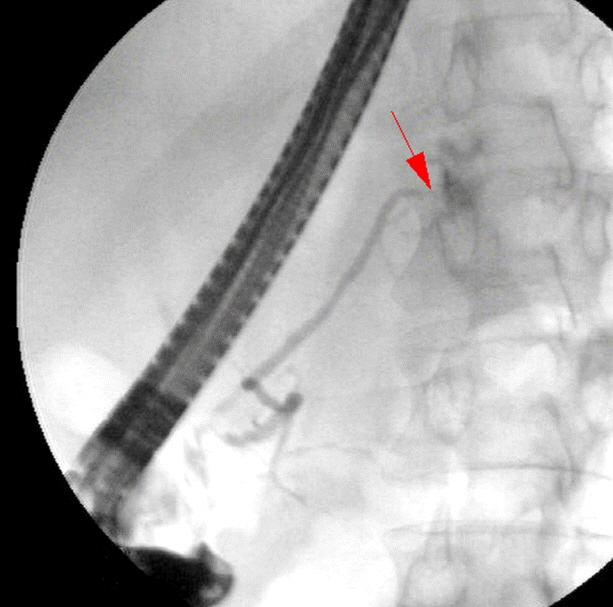
Fig. 2. Endoscopic retrograde cholangiopancreatography showing free outflow of the contrast medium from the proximal portion of the pancreatic tail to the mediastinum (the arrow points to the “leakage”).

Fig. 3. Endoscopic retrograde cholangiopancreatography showing the location of the stent in the pancreatic duct. The stent is placed distally to the fistula, as close as possible to the leakage point.
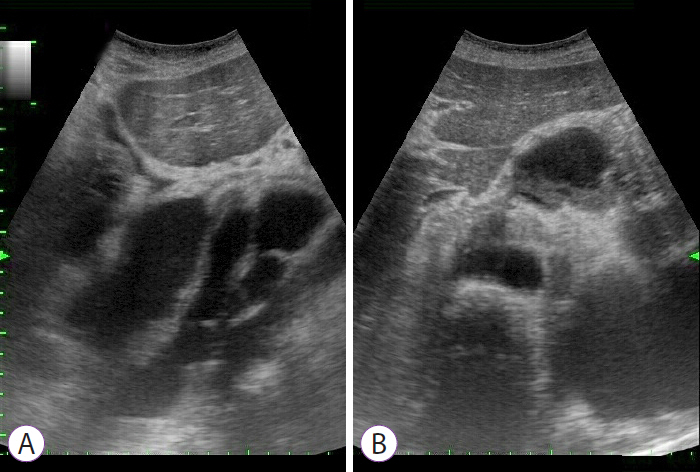
Fig. 4. (A, B) Abdominal ultrasound depicting pseudocysts in the posterior mediastinum.
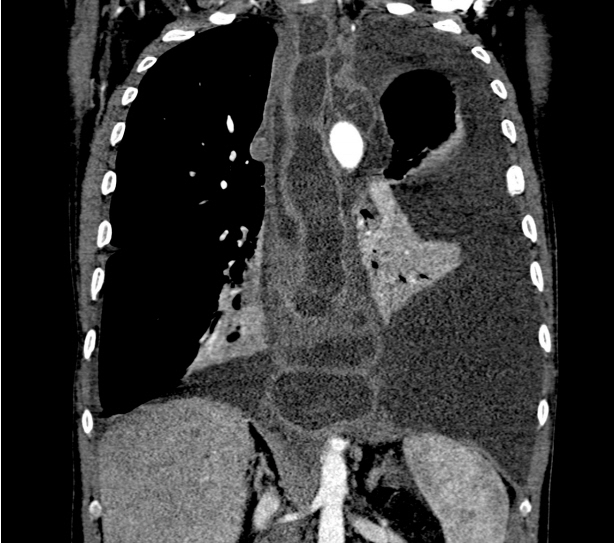
Fig. 5. Computed tomography scan of the chest showing mediastinal pseudocysts and pleural fluid.
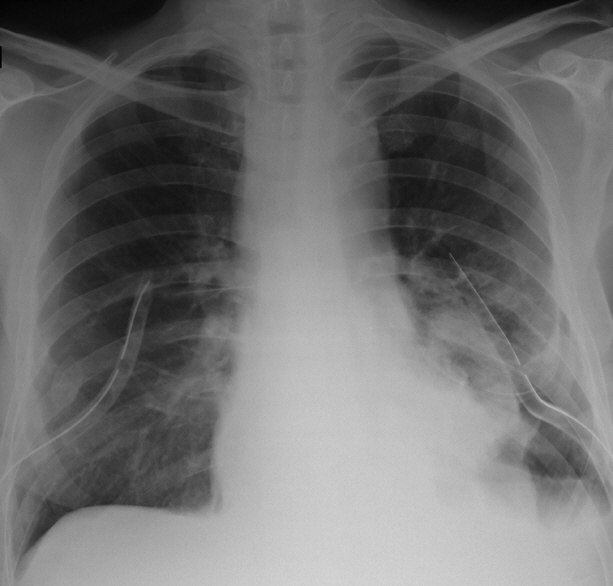
Fig. 6. Chest radiograph showing fluid resolution after pleural fluid drainage.

Fig. 7. Resolution of pseudocysts on the 12-month follow-up computed tomography scan.
Reference
-
1. Gupta R, Munoz JC, Garg P, Masri G, Nahman NS Jr, Lambiase LR. Mediastinal pancreatic pseudocyst: a case report and review of the literature. MedGenMed. 2007; 9:8.2. Dyrla P, Gil J, Wojtuń S, Florek M, Kasińska E, Zoń R. Pancreatic pseudocyst in the mediastinum. Pol Arch Med Wewn. 2014; 124:270–271.
Article3. Moorthy N, Raveesha A, Prabhakar K. Pancreaticopleural fistula and mediastinal pseudocyst: an unusual presentation of acute pancreatitis. Ann Thorac Med. 2007; 2:122–123.
Article4. Wronski M, Slodkowski M, Cebulski W, Moronczyk D, Krasnodebski IW. Optimizing management of pancreaticopleural fistulas. World J Gastroenterol. 2011; 17:4696–4703.
Article5. Dhebri AR, Ferran N. Nonsurgical management of pancreaticopleural fistula. JOP. 2005; 6:152–161.6. Altasan T, Aljehani Y, Almalki A, Algamdi S, Talag A, Alkattan K. Pancreaticopleural fistula: an overlooked entity. Asian Cardiovasc Thorac Ann. 2014; 22:98–101.
Article7. Ajmera AV, Judge TA. Mediastinal extension of pancreatic pseudocyst: a case with review of topic and management guidelines. Am J Ther. 2012; 19:e152–e156.8. Tay CM, Chang SK. Diagnosis and management of pancreaticopleural fistula. Singapore Med J. 2013; 54:190–194.
Article9. Safadi BY, Marks JM. Pancreatic-pleural fistula: the role of ERCP in diagnosis and treatment. Gastrointest Endosc. 2000; 51:213–215.
Article10. Suga H, Tsuruta O, Okabe Y, et al. A case of mediastinal pancreatic pseudocyst successfully treated with somatostatin analogue. Kurume Med J. 2005; 52:161–164.
Article11. Tsujimoto T, Takano M, Tsuruzono T, et al. Mediastinal pancreatic pseudocyst caused by obstruction of the pancreatic duct was eliminated by bromhexine hydrochloride. Intern Med. 2004; 43:1034–1038.
Article12. Ali T, Srinivasan N, Le V, Chimpiri AR, Tierney WM. Pancreaticopleural fistula. Pancreas. 2009; 38:e26–e31.
Article13. Belágyi T, Issekutz A, Paukovics A, Kecskés G, Oláh A. Successful treatment of mediastinal pancreatic pseudocyst by pancreatic head resection. JOP. 2008; 9:346–349.14. Takeuchi Y, Okabe H, Myojo S, Fujimoto S. CT-guided drainage of a mediastinal pancreatic pseudocyst with a transhepatic transdiaphragmatic approach. Hepatogastroenterology. 2002; 49:271–272.15. Săftoiu A, Ciurea T, Dumitrescu D, Stoica Z. Endoscopic ultrasound-guided transesophageal drainage of a mediastinal pancreatic pseudocyst. Endoscopy. 2006; 38:538–539.
Article16. Topa L, László F, Sahin P, Pozsár J. Endoscopic transgastric drainage of a pancreatic pseudocyst with mediastinal and cervical extensions. Gastrointest Endosc. 2006; 64:460–463.
Article17. Chang YC, Chen CW. Thoracoscopic drainage of ascending mediastinitis arising from pancreatic pseudocyst. Interact Cardiovasc Thorac Surg. 2009; 9:144–145.
Article18. Machado NO. Pancreaticopleural fistula: revisited. Diagn Ther Endosc. 2012; 2012:815476.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous Drainage of Pancreatic Pseudocysts: Analysis of 16 Cases
- Linear Array Endoscopic Ultrasound-Guided Drainage of a Pancreatic Pseudocyst without Using Fluoroscopy
- A Case of Mediastinal Pancreatic Pseudocyst
- Percutaneous drainage of pancreatic abscess and pseudocyst
- A Case of Pancreatic Pseudocyst Presenting as Duodenal Bleeding
