J Pathol Transl Med.
2015 May;49(3):262-266. 10.4132/jptm.2015.03.26.
Follicular Proliferative Lesion Arising in Struma Ovarii
- Affiliations
-
- 1Department of Pathology, Seoul National University College of Medicine, Seoul, Korea.
- 2Department of Pathology, Hallym University College of Medicine, Seoul, Korea.
- 3Department of Epidemiology and Preventive Medicine, Graduate School of Public Health, Seoul National University, Seoul, Korea. lilloa@snu.ac.kr
- KMID: 2381386
- DOI: http://doi.org/10.4132/jptm.2015.03.26
Abstract
- Malignant struma ovarii is extremely rare and difficult to diagnose histologically, particularly in cases of follicular carcinoma. This case study is intended to describe three cases of follicular proliferative lesion arising in struma ovarii that we experienced. The first case was clearly malignant given the clinical picture of multiple recurrences, but there was little histological evidence of malignancy. Our second case featured architectural and cellular atypia and necrosis and was diagnosed as malignant despite the absence of vascular and stromal invasion. Our third case exhibited solid microfollicular proliferation without any definite evidence of malignancy (even the molecular data was negative); however, we could not completely exclude malignant potential after conducting a literature review. In cases such as our third case, it has been previously suggested that a diagnostic term recognizing the low-grade malignant potential, such as "proliferative stromal ovarii" or "follicular proliferative lesion arising in the stromal ovarii" would be appropriate.
Figure
-
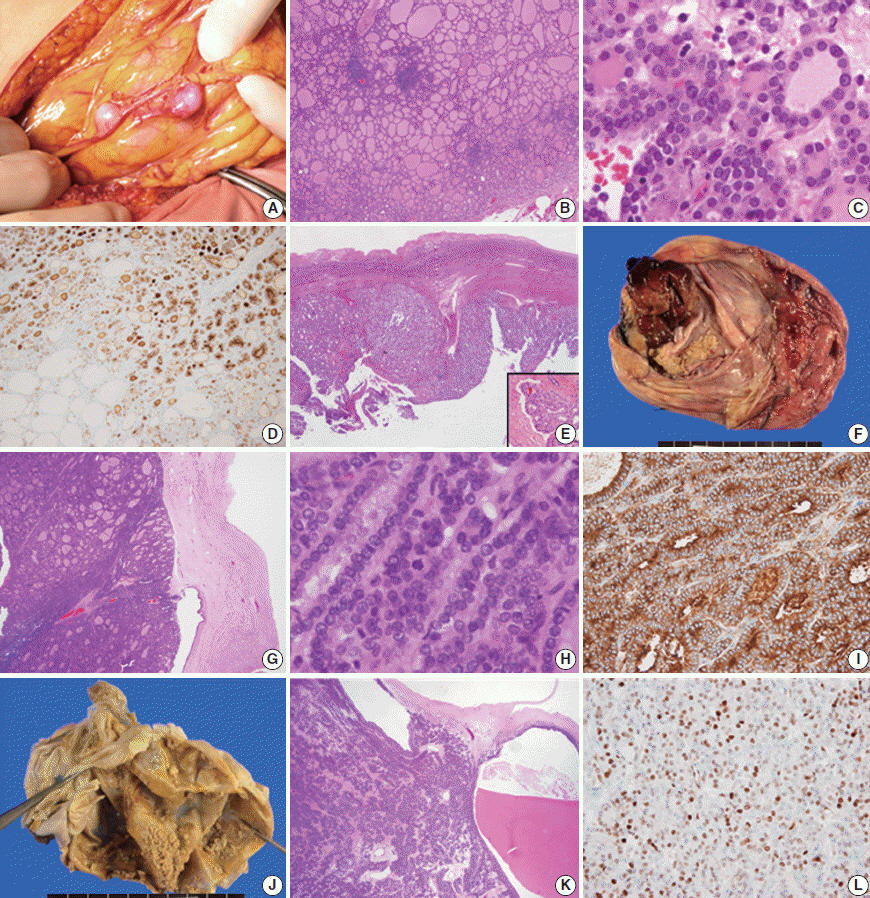
Fig. 1. Peritoneal nodules found intraoperatively (A) and the microscopic findings (B, C). HBME1 positivity of microfollicles of the first case (D) is observed and the initial ovarian lesion of the first case (E) shows vascular invasion (E, inset). The gross features of the second case (F) and the histological findings (G, H) are suggestive of malignancy, and HBME1 status is positive only in the cytoplasm (I). In the third case, the solid regions are tiny and scattered (J). Microscopically, microfollicles are predominant (K), and cyclin D1 expression is increased (L).
Reference
-
1. Kurman RJ, Carcangiu ML, Herrington CS, Young RH. WHO classification of tumours of female reproductive organs. 4th ed. Lyon: IARC Press;2014.2. Kurman RJ, Ellenson LH, Ronnett BM. Blaustein’s pathology of the female genital tract. 6th ed. New York: Springer;2010.3. Roth LM, Miller AW 3rd, Talerman A. Typical thyroid-type carcinoma arising in struma ovarii: a report of 4 cases and review of the literature. Int J Gynecol Pathol. 2008; 27:496–506.
Article4. Robboy SJ, Shaco-Levy R, Peng RY, et al. Malignant struma ovarii: an analysis of 88 cases, including 27 with extraovarian spread. Int J Gynecol Pathol. 2009; 28:405–22.
Article5. Zhang X, Axiotis C. Thyroid-type carcinoma of struma ovarii. Arch Pathol Lab Med. 2010; 134:786–91.
Article6. Roth LM, Talerman A. The enigma of struma ovarii. Pathology. 2007; 39:139–46.
Article7. Shaco-Levy R, Bean SM, Bentley RC, Robboy SJ. Natural history of biologically malignant struma ovarii: analysis of 27 cases with extraovarian spread. Int J Gynecol Pathol. 2010; 29:212–27.
Article8. Shaco-Levy R, Peng RY, Snyder MJ, et al. Malignant struma ovarii: a blinded study of 86 cases assessing which histologic features correlate with aggressive clinical behavior. Arch Pathol Lab Med. 2012; 136:172–8.
Article9. Roth LM, Karseladze AI. Highly differentiated follicular carcinoma arising from struma ovarii: a report of 3 cases, a review of the literature, and a reassessment of so-called peritoneal strumosis. Int J Gynecol Pathol. 2008; 27:213–22.10. Boutross-Tadross O, Saleh R, Asa SL. Follicular variant papillary thyroid carcinoma arising in struma ovarii. Endocr Pathol. 2007; 18:182–6.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Peritoneal dissemination of follicular carcinoma arising from struma ovarii in a pregnant woman
- A Case of Struma Ovarii
- Squamous Cell Carcinoma and Struma Ovarii Arising in Benign Cystic Teratoma
- Malignant struma ovarii with hyperthyroidism ; radionuclide study and treatment
- Squamous Cell Carcinoma and Struma Ovarii Arising in Benign Cystic Teratoma
