Implant placement simultaneously sinus augmentation using crestal approach in severely atrophic maxilla; minimally invasive approach
- Affiliations
-
- 1Department of Periodontology, School of Dentistry, Pusan National University, Yangsan, Republic of Korea. joojy@pusan.ac.kr
- KMID: 2377059
- DOI: http://doi.org/10.14368/jdras.2017.33.1.47
Abstract
- The atrophy of edentulous ridge and pneumatization of the maxillary sinus often limit the volume of bone available for implant placement on maxillary posterior teeth. Most clinicians suffer difficulties from poor bone quality and quantity on maxillary posterior site. Thus, the success of maxillary posterior implant surgery depends on the increase of the available bone and obtaining a good initial stability of the implant after maxillary sinus reconstruction. The maxillary sinus augmentation methods include a crestal approach and a lateral approach. Less morbidity and complications after operation is major advantage to sinus augmentation using crestal approach than lateral approach. However, when the residual ridge height is ≥ 6 mm, it is known that crestal approach is appropriate. Also delayed implantation after sinus augmentation is recommended in severely atrophic ridge. We present the three cases of implant placement simultaneously sinus augmentation using crestal approach in posterior maxilla site with ≤ 3 mm of residual alveolar bone.
MeSH Terms
Figure
-

Fig. 1 Radiographic findings of the 1st case. Left maxillary first molar was hopeless due to severe periodontitis (A). Residual bone height was 1.4 mm and bone quality was very poor on #26 site (B and C). Panorama view after #26 implantation (D).
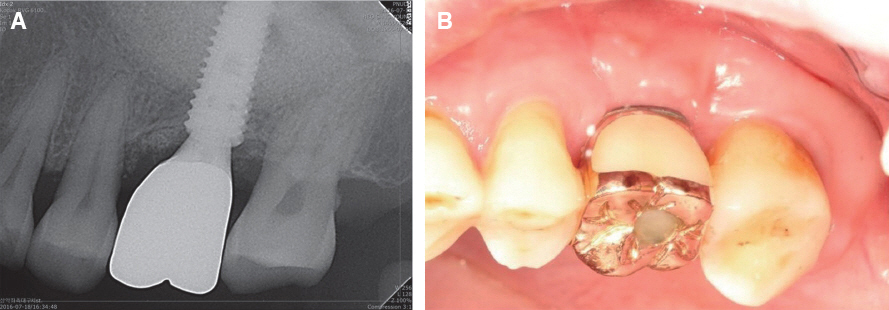
Fig. 2 Radiographic and clinical findings one year after #26i final prosthesis delivery. Marginal bone and augmented bone level was stable (A) and soft tissue was healthy (B).
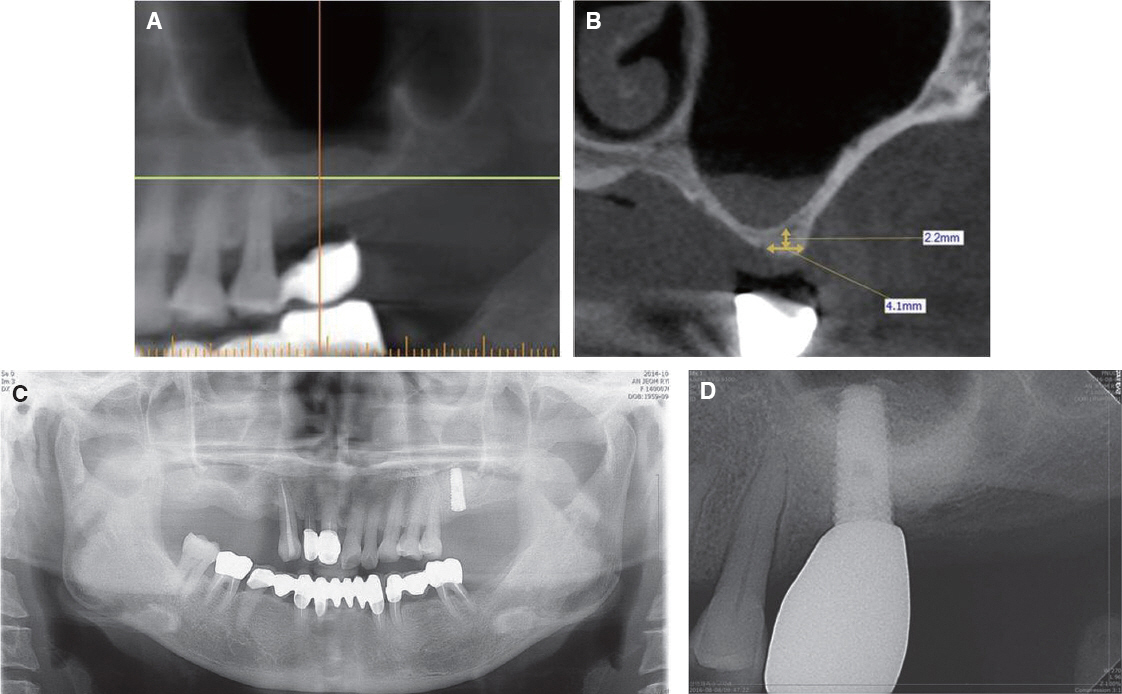
Fig. 3 Radiographic findings of the 2nd case. Residual bone height was 2.2 mm and schneiderian membrane was thicknening (A and B). Panorama view after #26 implantation (C). Marginal bone and augmented bone level was stable 1.5 year after final prosthesis delivery (D).
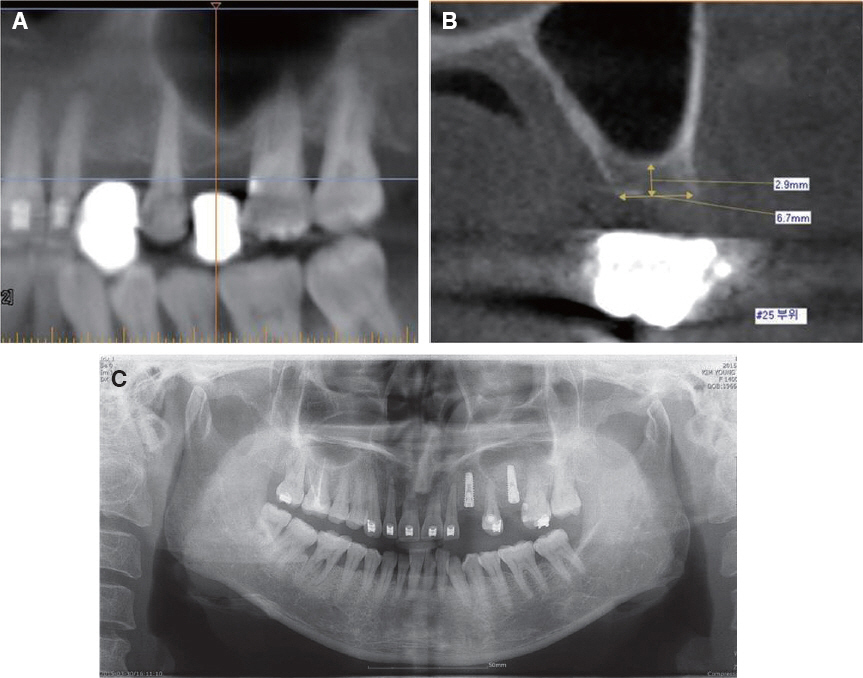
Fig. 4 Radiographic findings of the 3rd case. Residual bone height was 2.9 mm and poor bone quality was observed (A and B). Panorama view after #23 and #25 implantation (C).
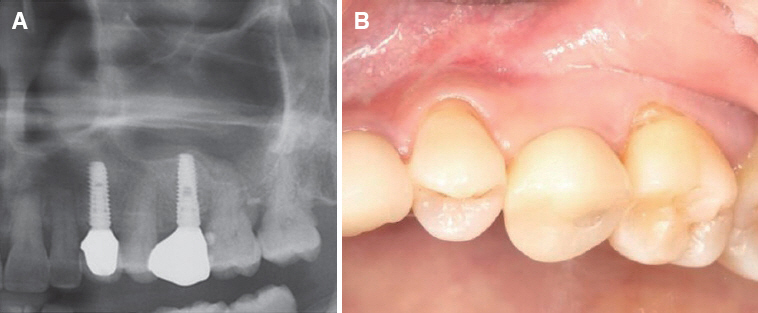
Fig. 5 Radiographic and clinical findings one year after #25i final prosthesis delivery. Marginal bone and augmented bone level was stable (A) and soft tissue was healthy (B).
Reference
-
References
1. Woo I, Le BT. Maxillary sinus floor elevation: review of anatomy and two techniques. Implant Dent. 2004; 13:28–32. DOI: 10.1097/01.ID.0000116369.66716.12. PMID: 15017301.2. Block MS. Improvements in the crestal osteotome approach have decreased the need for the lateral window approach to augment the maxilla. J Oral Maxillofac Surg. 2016; 74:2169–81. DOI: 10.1016/j.joms.2016.06.008. PMID: 27380546.3. Esposito M, Felice P, Worthington HV. Interventions for replacing missing teeth: augmentation procedures of the maxillary sinus. Cochrane Database Syst Rev. 2014; 5:CD008397. DOI: 10.1002/14651858.cd008397.pub2.4. Tallarico M, Meloni SM, Xhanari E, Pisano M, Cochran DL. Minimally invasive sinus augmentation procedure using a dedicated hydraulic sinus lift implant device: a prospective case series study on clinical, radiologic, and patient-centered outcomes. Int J Periodontics Restorative Dent. 2017; 37:125–35. DOI: 10.11607/prd.2914.5. Bruschi GB, Crespi R, Capparè P, Gherlone E. Transcrestal sinus floor elevation: a retrospective study of 46 patients up to 16 years. Clin Implant Dent Relat Res. 2012; 14:759–67. DOI: 10.1111/j.1708-8208.2010.00313.x. PMID: 20977614.6. Pjetursson BE, Ignjatovic D, Matuliene G, Brägger U, Schmidlin K, Lang NP. Transalveolar maxillary sinus floor elevation using osteotomes with or without grafting material. Part II: radiographic tissue remodeling. Clin Oral Implants Res. 2009; 20:67783. DOI: 10.1111/j.1600-0501.2009.01721.x. DOI: 10.1111/j.1600-0501.2009.01704.x. PMID: 19486079.7. Giannini S, Signorini L, Bonanome L, Severino M, Corpaci F, Cielo A. Benign paroxysmal positional vertigo (BPPV): it may occur after dental implantology. A mini topical review. Eur Rev Med Pharmacol Sci. 2015; 19:3543–7. PMID: 26502841.8. Better H, Slavescu D, Barbu H, Cochran DL, Chaushu G. Minimally invasive sinus lift implant device: a multicenter safety and efficacy trial preliminary results. Clin Implant Dent Relat Res. 2014; 16:520–6. DOI: 10.1111/cid.12021. PMID: 23190315.9. Kher U, Ioannou AL, Kumar T, Siormpas K, Mitsias ME, Mazor Z, Kotsakis GA. A clinical and radiographic case series of implants placed with the simplified minimally invasive antral membrane elevation technique in the posterior maxilla. J Craniomaxillofac Surg. 2014; 42:1942–7. DOI: 10.1016/j.jcms.2014.08.005. PMID: 25316651.10. Mazor Z, Kfir E, Lorean A, Mijiritsky E, Horowitz RA. Flapless approach to maxillary sinus augmentation using minimally invasive antral membrane balloon elevation. Implant Dent. 2011; 20:434–8. DOI: 10.1097/ID.0b013e3182391fe3. PMID: 22067602.11. Bataineh AB, Al-Dakes AM. The influence of length of implant on primary stability: an in vitro study using resonance frequency analysis. J Clin Exp Dent. 2017; 9:e1–e6. PMID: 28149455. PMCID: PMC5268121.12. Tan WC, Lang NP, Zwahlen M, Pjetursson BE. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. Part II: transalveolar technique. J Clin Periodontol. 2008; 35:24154. DOI: 10.1111/j.1600-051X.2008.01273.x. PMID: 18724853.13. Pjetursson BE, Lang NP. Sinus floor elevation utilizing the transalveolar approach. Periodontol 2000. 2014; 66:59–71. DOI: 10.1111/prd.12043. PMID: 25123761.14. Pjetursson BE, Tan WC, Zwahlen M, Lang NP. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. J Clin Periodontol. 2008; 35:216–40. DOI: 10.1111/j.1600-051X.2008.01272.x. PMID: 18724852.15. Lundgren S, Cricchio G, Hallman M, Jungner M, Rasmusson L, Sennerby L. Sinus floor elevation procedures to enable implant placement and integration: techniques, biological aspects and clinical outcomes. Periodontol 2000. 2017; 73:103–120. DOI: 10.1111/prd.12165. PMID: 28000271.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Installation Immediate Implant with Sinus Lift Crestal Approach Technique: A Case Report of 4-year Follow-up
- A Case of Implant Installation at Sinus Septa Using Sinus Crestal Approach: A 7-year Follow-up
- Stability of simultaneous implantation with autogenous iliac bone graft in the severely atrophic maxilla
- A Case of Surgical Technique to Overcome Vertical Bone Loss using a Resorbable Membrane with Fixation Screw and Sinus Crestal Approach: An 8-year Follow-up
- Radiographic change of grafted sinus floor after maxillary sinus floor elevation and placement of dental implant
