Yonsei Med J.
2016 Jul;57(4):1042-1046. 10.3349/ymj.2016.57.4.1042.
Unmasking Granulomatous Pneumocystis jirovecii Pneumonia with Nodular Opacity in an HIV-Infected Patient after Initiation of Antiretroviral Therapy
- Affiliations
-
- 1Division of Infectious Diseases, Department of Internal Medicine, Chungbuk National University Hospital, Cheongju, Korea. jyeon78@naver.com
- 2Department of Pathology, Chungbuk National University Hospital, Cheongju, Korea.
- 3Department of Radiology, Chungbuk National University Hospital, Cheongju, Korea.
- KMID: 2374142
- DOI: http://doi.org/10.3349/ymj.2016.57.4.1042
Abstract
- Pneumocystis jirovecii pneumonia (PJP) in patients with HIV infection can, in rare cases, present with pulmonary nodules that histologically involve granulomatous inflammation. This report describes an intriguing case of granulomatous PJP with pulmonary nodules after commencing antiretroviral therapy (ART) in an HIV-infected patient without respiratory signs or symptoms. Diagnosis of granulomatous PJP was only achieved through thoracoscopic lung biopsy. This case suggests that granulomatous PJP should be considered in the differential diagnosis of pulmonary nodules in HIV-infected patients for unmasking immune reconstitution inflammatory syndrome manifestation after initiation of ART.
Figure
-
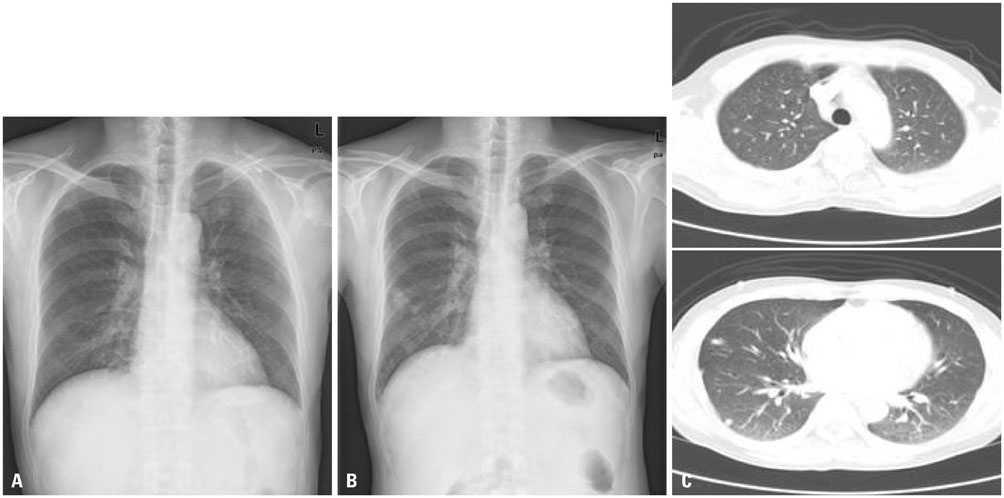
Fig. 1 (A) Plain chest radiograph within normal limits. (B) Plain chest radiograph showing newly developed multiple nodular lesions in the right lower lung field. (C) Chest CT scans showing multiple nodular lesions in the right and left lower lobes of the lung.

Fig. 2 (A) Chronic granulomatous inflammation seen in the lung parenchyma, which filled with secretory materials in alveolar spaces (hematoxylin and eosin stain, ×200). (B) Pneumocystis jirovecii cysts, 5–8 µm in size, seen with an alveolar plaque stained using Gomori methenamine silver stain (×800).
Reference
-
1. Travis WD, Pittaluga S, Lipschik GY, Ognibene FP, Suffredini AF, Masur H, et al. Atypical pathologic manifestations of Pneumocystis carinii pneumonia in the acquired immune deficiency syndrome. Review of 123 lung biopsies from 76 patients with emphasis on cysts, vascular invasion, vasculitis, and granulomas. Am J Surg Pathol. 1990; 14:615–625.
Article2. Hartel PH, Shilo K, Klassen-Fischer M, Neafie RC, Ozbudak IH, Galvin JR, et al. Granulomatous reaction to pneumocystis jirovecii: clinicopathologic review of 20 cases. Am J Surg Pathol. 2010; 34:730–734.3. Totet A, Duwat H, Daste G, Berry A, Escamilla R, Nevez G. Pneumocystis jirovecii genotypes and granulomatous pneumocystosis. Med Mal Infect. 2006; 36:229–231.4. Gilroy SA, Bennett NJ. Pneumocystis pneumonia. Semin Respir Crit Care Med. 2011; 32:775–782.
Article5. Autran B, Carcelain G, Li TS, Blanc C, Mathez D, Tubiana R, et al. Positive effects of combined antiretroviral therapy on CD4+ T cell homeostasis and function in advanced HIV disease. Science. 1997; 277:112–116.
Article6. Blumenfeld W, Basgoz N, Owen WF Jr, Schmidt DM. Granulomatous pulmonary lesions in patients with the acquired immunodeficiency syndrome (AIDS) and Pneumocystis carinii infection. Ann Intern Med. 1988; 109:505–507.
Article7. Klein JS, Warnock M, Webb WR, Gamsu G. Cavitating and noncavitating granulomas in AIDS patients with Pneumocystis pneumonitis. AJR Am J Roentgenol. 1989; 152:753–754.
Article8. Birley HD, Buscombe JR, Griffiths MH, Semple SJ, Miller RF. Granulomatous Pneumocystis carinii pneumonia in a patient with the acquired immunodeficiency syndrome. Thorax. 1990; 45:769–771.
Article9. Flannery MT, Quiroz E, Grundy LS, Brantley S. Pneumocystis carinii pneumonia with an atypical granulomatous response. South Med J. 1996; 89:409–410.
Article10. Takahashi T, Nakamura T, Iwamoto A. Reconstitution of immune responses to Pneumocystis carinii pneumonia in patients with HIV infection who receive highly active antiretroviral therapy. Res Commun Mol Pathol Pharmacol. 2002; 112:59–67.11. Chen F, Sethi G, Goldin R, Wright AR, Lacey CJ. Concurrent granulomatous Pneumocystis carinii and Mycobacterium xenopi pneumonia: an unusual manifestation of HIV immune reconstitution disease. Thorax. 2004; 59:997–999.
Article12. Sabur N, Kelly MM, Gill MJ, Ainslie MD, Pendharkar SR. Granulomatous Pneumocystis jiroveci pneumonia associated with immune reconstituted HIV. Can Respir J. 2011; 18:e86–e88.
Article13. Wu AK, Cheng VC, Tang BS, Hung IF, Lee RA, Hui DS, et al. The unmasking of Pneumocystis jiroveci pneumonia during reversal of immunosuppression: case reports and literature review. BMC Infect Dis. 2004; 4:57.
Article14. Müller M, Wandel S, Colebunders R, Attia S, Furrer H, Egger M. Ie-DEA Southern and Central Africa. Immune reconstitution inflammatory syndrome in patients starting antiretroviral therapy for HIV infection: a systematic review and meta-analysis. Lancet Infect Dis. 2010; 10:251–261.
Article15. Calderón EJ, Gutiérrez-Rivero S, Durand-Joly I, Dei-Cas E. Pneumocystis infection in humans: diagnosis and treatment. Expert Rev Anti Infect Ther. 2010; 8:683–701.16. Lundberg BE, Davidson AJ, Burman WJ. Epidemiology of Pneumocystis carinii pneumonia in an era of effective prophylaxis: the relative contribution of non-adherence and drug failure. AIDS. 2000; 14:2559–2566.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Extracorporeal Membrane Oxygenation for Acute Respiratory Distress Syndrome following HAART Initiation in an HIV-infected Patient Being Treated for Severe Pneumocystis jirovecii Pneumonia: Case Report and Literature Review
- Single Nodular Opacity of Granulomatous Pneumocystis Jirovecii Pneumonia in an Asymptomatic Lymphoma Patient
- Pneumocystis jirovecii Pneumonia Accompanied with Fat Embolism: A Case Report
- A Case of Pneumonia Caused by Pneumocystis jirovecii Resistant to Trimethoprim/Sulfamethoxazole in the Absence of Previous Drug Exposure
- Pneumocystis jirovecii Pneumonia with Granulomatous Reaction in the Lung and the Liver Discovered at Autopsy
