Is There Any Age Cutoff to Treat Elderly Patients with Head and Neck Cancer? Comparing with Septuagenarians and Octogenarians
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Hallym University, Dongtan Sacred Heart Hospital, Hwaseong, Korea.
- 2Department of Otorhinolaryngology-Head and Neck Surgery, Seoul National University College of Medicine, Seoul, Korea. jhunhah@snu.ac.kr
- 3Cancer Research Institute, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2373760
- DOI: http://doi.org/10.3346/jkms.2016.31.8.1300
Abstract
- With the increase in life expectancy, age is no longer considered as a limitation for treatment. Nevertheless, the treatment of elderly patients with head and neck cancer (HNC) remains controversial. Here, we aimed to review our experience with the treatment for elderly patients, while particularly focusing on the differences among older old patients (septuagenarians vs. octogenarians). We retrospectively reviewed the records of 260 elderly patients who were assigned to 3 groups according to age: 70 years old ≤ group 1 < 75 years old, 75 years old ≤ group 2 < 80 years old, and group 3 ≥ 80 years old. The patients were assessed for comorbidities using the Adult Comorbidity Evaluation (ACE)-27, and the American Society of Anesthesia (ASA) physical status was also compared. Group 1, 2, and 3, consisted of 97, 102, and 61 patients, respectively. No significant difference in demographic data was noted among the groups. However, group 3 showed more comorbidities than groups 1 and 2. With regard to the initial treatment for HNC, radiation therapy (RT) was more frequently performed in group 3 than in groups 1 and 2. Among 7 patients of non-compliant to treatment in group 3, 6 patients had have performed RT. In group 3, a total of 18 patients underwent surgery, including microvascular free flap reconstruction and no significant difference in complications was observed postoperatively compared with group 1 and 2. Moreover, no significant difference was noted in overall survival between the groups, regardless of the treatment modality chosen. In conclusion, octogenarians with HNC should be more carefully managed than septuagenarians with HNC. Surgical treatment can be considered in octogenarians with HNC, if it can be tolerated.
Keyword
MeSH Terms
Figure
-
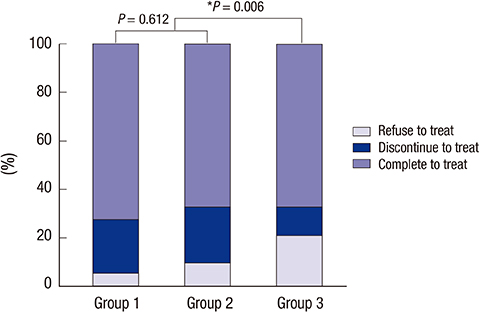
Fig. 1 The differences in treatment compliance ratios between septuagenarian and octogenarian head and neck cancer patients (Group 1: 70-75 years, Group 2: 76-80 years, Group 3: 80 years and older).
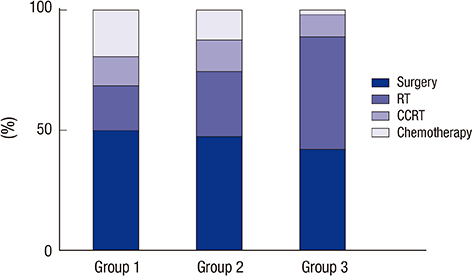
Fig. 2 The percentages of treatment modalities which were chosen for initial treatment for their head and neck cancer.
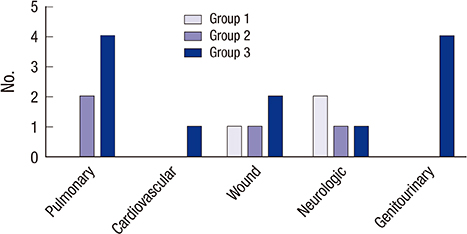
Fig. 3 Major and minor complications occurring within 1 week after surgery in elderly head and neck cancer patients.

Fig. 4 Overall survival of elderly patients with head and neck cancer (HNC) following therapeutic intervention. (A) Overall survival of patients who completed treatment for HNC, excluding patients who ceased during treatment. (B) Overall Survival of patients who underwent surgery for their HNC; Group 1 & 2 (septuagenarians) vs. Group 3 (octogenarians).
Reference
-
1. Organisation for Economic Co-operation and Development. Health Status [Internet]. accessed on 29 July 2015. Available at http://stats.oecd.org/index.aspx?DataSetCode=HEALTH_STAT#.2. Muir CS, Fraumeni JF Jr, Doll R. The interpretation of time trends. Cancer Surv. 1994; 19-20:5–21.3. Olmi P, Ausili-Cefaro G. Radiotherapy in the elderly: a multicentric prospective study on 2060 patients referred to 37 Italian radiation therapy centers. Rays. 1997; 22:53–56.4. Balducci L. Management of cancer in the elderly. Oncology (Williston Park). 2006; 20:135–143.5. Mountzios G. Optimal management of the elderly patient with head and neck cancer: issues regarding surgery, irradiation and chemotherapy. World J Clin Oncol. 2015; 6:7–15.6. Pignon T, Horiot JC, Van den Bogaert W, Van Glabbeke M, Scalliet P. No age limit for radical radiotherapy in head and neck tumours. Eur J Cancer. 1996; 32:2075–2081.7. Ang KK, Harris J, Wheeler R, Weber R, Rosenthal DI, Nguyen-Tân PF, Westra WH, Chung CH, Jordan RC, Lu C, et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med. 2010; 363:24–35.8. Koch WM, Patel H, Brennan J, Boyle JO, Sidransky D. Squamous cell carcinoma of the head and neck in the elderly. Arch Otolaryngol Head Neck Surg. 1995; 121:262–265.9. Jones PA. DNA methylation errors and cancer. Cancer Res. 1996; 56:2463–2467.10. Italiano A, Ortholan C, Dassonville O, Poissonnet G, Thariat J, Benezery K, Vallicioni J, Peyrade F, Marcy PY, Bensadoun RJ. Head and neck squamous cell carcinoma in patients aged ≥ 80 years: patterns of care and survival. Cancer. 2008; 113:3160–3168.11. Teymoortash A, Wulf H, Werner JA. Head and neck cancer surgery in the elderly. Laryngorhinootologie. 2002; 81:293–298.12. McGuirt WF, Loevy S, McCabe BF, Krause CJ. The risks of major head and neck surgery in the aged population. Laryngoscope. 1977; 87:1378–1382.13. Piccirillo JF. Importance of comorbidity in head and neck cancer. Laryngoscope. 2000; 110:593–602.14. Thomas M, George NA, Gowri BP, George PS, Sebastian P. Comparative evaluation of ASA classification and ACE-27 index as morbidity scoring systems in oncosurgeries. Indian J Anaesth. 2010; 54:219–225.15. Ferrier MB, Spuesens EB, Le Cessie S, Baatenburg de Jong RJ. Comorbidity as a major risk factor for mortality and complications in head and neck surgery. Arch Otolaryngol Head Neck Surg. 2005; 131:27–32.16. Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010; 17:1471–1474.17. Sarris EG, Harrington KJ, Saif MW, Syrigos KN. Multimodal treatment strategies for elderly patients with head and neck cancer. Cancer Treat Rev. 2014; 40:465–475.18. Vercelli M, Parodi S, Serraino D. Overall cancer incidence and mortality trends among elderly and adult Europeans. Crit Rev Oncol Hematol. 1998; 27:87–96.19. Wedding U, Bokemeyer C, Meran JG; Working Group Geriatric Oncology of the German Society for Haematology and Oncology (DGHO). Austrian Society for Haematology and Oncology (OGHO); German Society for Geriatrics (DGG). Elderly patients with acute myeloid leukaemia: characteristics in biology, patients and treatment. Recommendations of the Working Group Geriatric Oncology of the German Society for Haematology and Oncology (DGHO), the Austrian Society for Haematology and Oncology (OGHO) and the German Society for Geriatrics (DGG). Onkologie. 2004; 27:72–82.20. Balducci L. Geriatric oncology: challenges for the new century. Eur J Cancer. 2000; 36:1741–1754.21. Derks W, de Leeuw JR, Hordijk GJ, Winnubst JA. Reasons for non-standard treatment in elderly patients with advanced head and neck cancer. Eur Arch Otorhinolaryngol. 2005; 262:21–26.22. Yamakawa M, Shiojima K, Takahashi M, Saito Y, Matsumoto H, Mitsuhashi N, Niibe H. Radiation therapy for esophageal cancer in patients over 80 years old. Int J Radiat Oncol Biol Phys. 1994; 30:1225–1232.23. Schilcher B, Curschmann J. Clinical results of radiotherapy in 140 elderly patients treated at Basel University Hospital between 1980 and 1985. Int J Radiat Oncol Biol Phys. 1995; 33:774.24. Sharma A, Madan R, Kumar R, Sagar P, Kamal VK, Thakar A, Sharma A, Mohanti BK. Compliance to therapy-elderly head and neck carcinoma patients. Can Geriatr J. 2014; 17:83–87.25. Howard MA, Cordeiro PG, Disa J, Samson W, Gonen M, Schoelle RN, Mehrara B. Free tissue transfer in the elderly: incidence of perioperative complications following microsurgical reconstruction of 197 septuagenarians and octogenarians. Plast Reconstr Surg. 2005; 116:1659–1668.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Off-Pump Coronary Artery Bypass between Octogenarians and Septuagenarians: A Propensity Score Analysis
- The Clinical Impact of Advanced Age on the Postoperative Outcomes of Patients Undergoing Gastrectomy for Gastric Cancer: Analysis Across US Hospitals Between 2011–2017
- Surgical outcomes and prognostic factors of gastric cancer surgery in octogenarians
- Frailty in Geriatric Patients with Head and Neck Cancer and its Implication in Survivorship
- Determination of Diagnosis and Treatment for Head and Neck Cancer Patients Considering Frailty
