J Gastric Cancer.
2010 Jun;10(2):84-86.
Laparoscopic Surgery for Removal of the Multiple Large Gastric Bezoars
- Affiliations
-
- 1Department of Surgery, Incheon St. Mary's Hospital, The Catholic University of Korea, Incheon, Korea. parksm@catholic.ac.kr
Abstract
- Bezoars are retained concretions of undigested animal or vegetable material that can produce gastrointestinal obstruction, ulceration, and bleeding. Therapeutic options for gastric bezoars include enzyme therapy (papain, cellulase, or acetylcysteine), endoscopic disruption and removal, and surgical removal. Multiple large gastric bezoars generally require conventional surgical management through an upper abdominal incision. With the recent improvement of laparoscopy, a lot of portions of abdominal operations have been performed laparoscopically. We successfully removed multiple large gastric phytobezoars in a 52-year-old female completely through laparoscopy. This supported the feasibility of laparoscopic surgery for patients with gastric bezoars.
Keyword
MeSH Terms
Figure
-
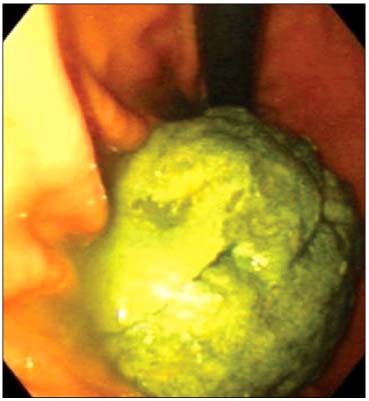
Fig. 1 Gastroscopic finding. Gastroscopic finding showed multiple large gastric bezoar.

Fig. 2 Intraoperative view of laparoscopic removal for gastric bezoars. The bezoars were extracted through a gastrotomy on the anterior wall of the gastric body and placed directly in the endo-bag without any spillage.

Fig. 3 Specimens of fragmented bezoars. The bezoars were morcellated and removed in fragments.

Fig. 4 Intraoperative view of laparoscopic gastrotomy closure. The gastrotomy site was closed using endo-GIA staplers after the placement of stay sutures.
Reference
-
1. de Menezes Ettinger JE, Silva Reis JM, de Souza EL, Filho Ede M, Gãlvao do Amaral PC, Ettinger E Jr, et al. Laparoscopic management of intestinal obstruction due to phytobezoar. JSLS. 2007. 11:168–171.2. Robles R, Lujan JA, Parrilla P, Torralba JA, Escamilla C. Laparoscopic surgery in the treatment of small bowel obstruction by bezoar. Br J Surg. 1995. 82:520.
Article3. Andrus CH, Ponsky JL. Bezoars: classification, pathophysiology, and treatment. Am J Gastroenterol. 1988. 83:476–478.4. Coulter R, Antony MT, Bhuta P, Memon MA. Large gastric trichobezoar in a normal healthy woman: case report and review of pertinent literature. South Med J. 2005. 98:1042–1044.
Article5. Kuo JY, Mo LR, Tsai CC, Chou CY, Lin RC, Chang KK. Nonoperative treatment of gastric bezoars using electrohydraulic lithotripsy. Endoscopy. 1999. 31:386–388.
Article6. Wang YG, Seitz U, Li ZL, Soehendra N, Qiao XA. Endoscopic management of huge bezoars. Endoscopy. 1998. 30:371–374.
Article7. Naveau S, Poynard T, Zourabichvili O, Poitrine A, Chaput JC. Gastric phytobezoar destruction by Nd:YAG laser therapy. Gastrointest Endosc. 1986. 32:430–431.
Article8. Nirasawa Y, Mori T, Ito Y, Tanaka H, Seki N, Atomi Y. Laparoscopic removal of a large gastric trichobezoar. J Pediatr Surg. 1998. 33:663–665.
Article9. Yau KK, Siu WT, Law BK, Cheung HY, Ha JP, Li MK. Laparoscopic approach compared with conventional open approach for bezoar-induced small-bowel obstruction. Arch Surg. 2005. 140:972–975.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Megaduodenum with Duodenal Diospyrobezoars
- Laparoscopic Removal of a Gastric Trichobezoar in an 8-Year-Old Girl: a Case Report
- New Surgical Approach for Gastric Bezoar: "Hybrid Access Surgery" Combined Intragastric and Single Port Surgery
- The Intestinal Obstruction Due to Bezoar
- The Successful Dissolution of 2 Cases of Fat Bezoars by Pancreatic Lipase
