Laparoscopic Total Gastrectomy in a Gastric Cancer Patient with Intestinal Malrotation
- Affiliations
-
- 1Department of Surgery, Yonsei University College of Medicine, Seoul, Korea. wjhyung@yuhs.ac
- 2Department of Radiology, Yonsei University College of Medicine, Seoul, Korea.
- 3Gastric Cancer Clinic, Severance Hospital, Yonsei University Health System, Seoul, Korea.
- 4Robot and MIS Center, Severance Hospital, Yonsei University Health System, Seoul, Korea.
Abstract
- As the incidence of early gastric cancer increases, laparoscopic surgery has become one of the treatments of choice for gastric cancer. With the increase of laparoscopic surgery, the chance of discovering aberrant anatomy during the operation also increases. We present a case of laparoscopic total gastrectomy in gastric cancer patients with intestinal malrotation. Intestinal malrotation occurs in one in every 500 births. We found that laparoscopic total gastrectomy in such patients can be performed successfully when it is performed with a proper Roux limb orientation through an alternative minilaparotomy.
MeSH Terms
Figure
-

Fig. 1 Preoperative evaluation. (A) Esophagogastroduodenoscopy. (B) Computed tomography axial view. Small bowel is located on the right side of the abdomen. The superior mesenteric vein (long white arrow) is located on the left side of the superior mesenteric artery (short white arrow). (C) Coronal view. Ileocecal valve (arrow) is on the left side of the abdomen.
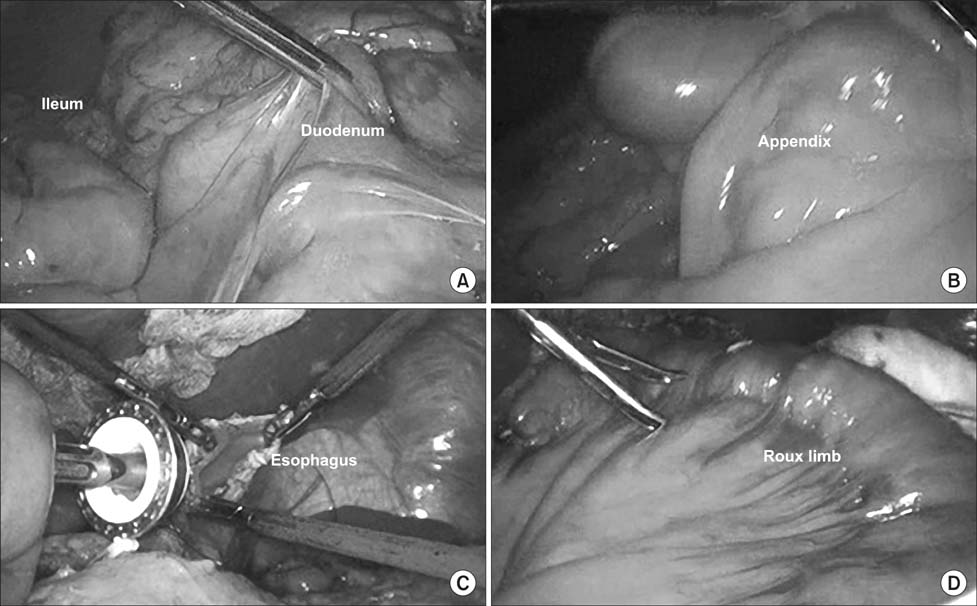
Fig. 2 Operative findings. (A) Small bowel on the right side. (B) Appendix is found on the left side of the abdomen. (C) Anvil approach for esophagojejunostomy. (D) Roux limb in clockwise rotation.
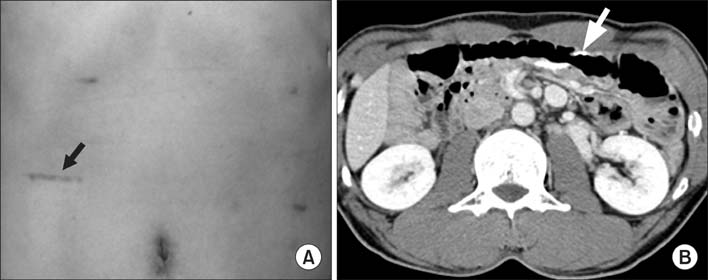
Fig. 3 (A) The modified minilaparotomy scar (arrow) on the right lower abdomen. (B) Follow-up computed tomography (CT) shows jejunojejunostomy (arrow) in the left side of the abdomen.
Reference
-
1. Kapfer SA, Rappold JF. Intestinal malrotation-not just the pediatric surgeon's problem. J Am Coll Surg. 2004; 199:628–635.
Article2. Hyung WJ, Lim JS, Song J, Choi SH, Noh SH. Laparoscopic spleen-preserving splenic hilar lymph node dissection during total gastrectomy for gastric cancer. J Am Coll Surg. 2008; 207:e6–e11.3. Kim HI, Cho I, Jang DS, Hyung WJ. Intracorporeal esophagojejunostomy using a circular stapler with a new purse-string suture technique during laparoscopic total gastrectomy. J Am Coll Surg. 2013; 216:e11–e16.
Article4. Gohl ML, DeMeester TR. Midgut nonrotation in adults. An aggressive approach. Am J Surg. 1975; 129:319–323.5. Stewart DR, Colodny AL, Daggett WC. Malrotation of the bowel in infants and children: a 15 year review. Surgery. 1976; 79:716–720.6. Swenson O, Ladd WE. Surgical emergencies of the alimentary tract of the newborn. N Engl J Med. 1945; 233:660–663.
Article7. Gilbert HW, Armstrong CP, Thompson MH. The presentation of malrotation of the intestine in adults. Ann R Coll Surg Engl. 1990; 72:239–242.8. Spigland N, Brandt ML, Yazbeck S. Malrotation presenting beyond the neonatal period. J Pediatr Surg. 1990; 25:1139–1142.
Article9. Jeong GA, Cho GS, Kim HH, Lee HJ, Ryu SW, Song KY. Laparoscopy-assisted total gastrectomy for gastric cancer: a multicenter retrospective analysis. Surgery. 2009; 146:469–474.
Article10. Park DJ, Han SU, Hyung WJ, Kim MC, Kim W, Ryu SY, et al. Long-term outcomes after laparoscopy-assisted gastrectomy for advanced gastric cancer: a large-scale multicenter retrospective study. Surg Endosc. 2012; 26:1548–1553.
Article11. Lee MS, Lee JH, Park do J, Lee HJ, Kim HH, Yang HK. Comparison of short- and long-term outcomes of laparoscopicassisted total gastrectomy and open total gastrectomy in gastric cancer patients. Surg Endosc. 2013; 27:2598–2605.
Article12. Matzke GM, Dozois EJ, Larson DW, Moir CR. Surgical management of intestinal malrotation in adults: comparative results for open and laparoscopic Ladd procedures. Surg Endosc. 2005; 19:1416–1419.
Article13. Draus JM Jr, Foley DS, Bond SJ. Laparoscopic Ladd procedure: a minimally invasive approach to malrotation without midgut volvulus. Am Surg. 2007; 73:693–696.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intracorporeal Anastomosis in Laparoscopic Gastric Cancer Surgery
- Laparoscopic Surgery for Advanced Gastric Cancer: Current Status and Future Perspectives
- Entirely Laparoscopic Gastrectomy and Colectomy for Remnant Gastric Cancer with Gastric Outlet Obstruction and Transverse Colon Invasion
- Two Cases of Laparoscopic Adhesiolysis for Chronic Abdominal Pain without Intestinal Obstruction after Total Gastrectomy
- Single-Port Laparoscopic Proximal Gastrectomy with Double Tract Reconstruction for Early Gastric Cancer: Report of a Case
