Comparison of Surgical Outcomes between Robotic and Laparoscopic Gastrectomy for Gastric Cancer: The Learning Curve of Robotic Surgery
- Affiliations
-
- 1Department of Surgery, Ajou University School of Medicine, Suwon, Korea. hansu@ajou.ac.kr
Abstract
- PURPOSE
Laparoscopic gastrectomy is a widely accepted surgical technique. Recently, robotic gastrectomy has been developed, as an alternative minimally invasive surgical technique. This study aimed to evaluate the question of whether robotic gastrectomy is feasible and safe for the treatment of gastric cancer, due to its learning curve.
MATERIALS AND METHODS
We retrospectively reviewed the prospectively collected data of 100 consecutive robotic gastrectomy patients, from November 2008 to March 2011, and compared them to 282 conventional laparoscopy patients during the same period. The robotic gastrectomy patients were divided into 20 initial cases; and all subsequent cases; and we compared the clinicopathological features, operating times, and surgical outcomes between the three groups.
RESULTS
The initial 20 robotic gastrectomy cases were defined as the initial group, due to the learning curve. The initial group had a longer average operating time (242.25+/-74.54 minutes vs. 192.56+/-39.56 minutes, P>0.001), and hospital stay (14.40+/-24.93 days vs. 8.66+/-5.39 days, P=0.001) than the experienced group. The length of hospital stay was no different between the experienced group, and the laproscopic gastrectomy group (8.66+/-5.39 days vs. 8.11+/-4.10 days, P=0.001). The average blood loss was significantly less for the robotic gastrectomy groups, than for the laparoscopic gastrectomy group (93.25+/-84.59 ml vs. 173.45+/-145.19 ml, P<0.001), but the complication rates were no different.
CONCLUSIONS
Our study shows that robotic gastrectomy is a safe and feasible procedure, especially after the 20 initial cases, and provides a satisfactory postoperative outcome.
Keyword
MeSH Terms
Figure
-

Fig. 1 Trocar insertion in a robotic gastrectomy case (right) and laparoscopic case (left). The robotic case had lower trocar sites than the laparoscopic case.

Fig. 2 The mean operating times of 10 sequential patients from the initial cases of robotic gastrectomy (error bars represent standard error).
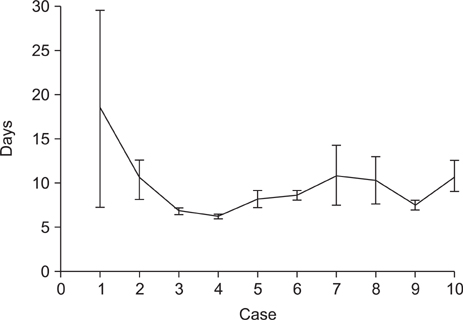
Fig. 3 The mean lengths of hospital stay of 10 sequential patients from the initial cases of robotic gastrectomy (error bars represent standard error).
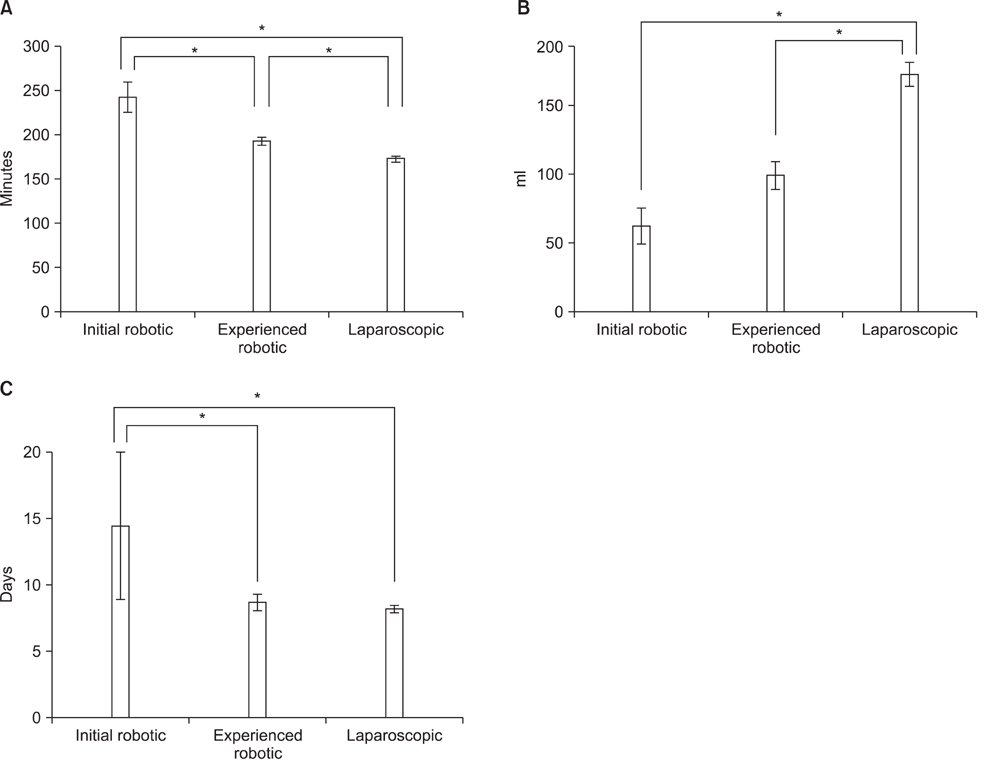
Fig. 4 (A) Comparison of the operating time among initial robotic, experienced robotic and laparoscopic gastrectpmy groups. (B) Comparison of the blood loss during the operation among the initial robotic, experienced robotic and laparoscopic gastrectomy groups. (C) Comparison of the length of hospital stay among the initial robotic, experienced robotic and laparoscopic gastrectomy groups. *Means P<0.05 by Tukey's honestly significant difference post-hoc test. Error bars represent standard error.
Reference
-
1. Shin HR, Jung KW, Won YJ, Kong HJ, Yim SH, Sung J, et al. National cancer incidence for the year 2002 in Korea. Cancer Res Treat. 2007. 39:139–149.
Article2. Ahn HS, Lee HJ, Yoo MW, Jeong SH, Park DJ, Kim HH, et al. Changes in clinicopathological features and survival after gastrectomy for gastric cancer over a 20-year period. Br J Surg. 2011. 98:255–260.
Article3. Kim MC, Kim W, Kim HH, Ryu SW, Ryu SY, Song KY, et al. Korean Laparoscopic Gastrointestinal Surgery Study (KLASS) Group. Risk factors associated with complication following laparoscopy-assisted gastrectomy for gastric cancer: a large-scale korean multicenter study. Ann Surg Oncol. 2008. 15:2692–2700.
Article4. Shehzad K, Mohiuddin K, Nizami S, Sharma H, Khan IM, Memon B, et al. Current status of minimal access surgery for gastric cancer. Surg Oncol. 2007. 16:85–98.
Article5. Kitano S, Shiraishi N, Uyama I, Sugihara K, Tanigawa N. Japanese Laparoscopic Surgery Study Group. A multicenter study on oncologic outcome of laparoscopic gastrectomy for early cancer in Japan. Ann Surg. 2007. 245:68–72.
Article6. Kim MC, Heo GU, Jung GJ. Robotic gastrectomy for gastric cancer: surgical techniques and clinical merits. Surg Endosc. 2010. 24:610–615.
Article7. Cadière GB, Himpens J, Germay O, Izizaw R, Degueldre M, Vandromme J, et al. Feasibility of robotic laparoscopic surgery: 146 cases. World J Surg. 2001. 25:1467–1477.8. Lanfranco AR, Castellanos AE, Desai JP, Meyers WC. Robotic surgery: a current perspective. Ann Surg. 2004. 239:14–21.9. Song J, Oh SJ, Kang WH, Hyung WJ, Choi SH, Noh SH. Robot-assisted gastrectomy with lymph node dissection for gastric cancer: lessons learned from an initial 100 consecutive procedures. Ann Surg. 2009. 249:927–932.
Article10. Pugliese R, Maggioni D, Sansonna F, Ferrari GC, Forgione A, Costanzi A, et al. Outcomes and survival after laparoscopic gastrectomy for adenocarcinoma. Analysis on 65 patients operated on by conventional or robot-assisted minimal access procedures. Eur J Surg Oncol. 2009. 35:281–288.
Article11. Woo Y, Hyung WJ, Pak KH, Inaba K, Obama K, Choi SH, et al. Robotic gastrectomy as an oncologically sound alternative to laparoscopic resections for the treatment of early-stage gastric cancers. Arch Surg. 2011. 146:1086–1092.
Article12. Anderson C, Ellenhorn J, Hellan M, Pigazzi A. Pilot series of robot-assisted laparoscopic subtotal gastrectomy with extended lymphadenectomy for gastric cancer. Surg Endosc. 2007. 21:1662–1666.
Article13. Patriti A, Ceccarelli G, Bellochi R, Bartoli A, Spaziani A, Di Zitti L, et al. Robot-assisted laparoscopic total and partial gastric resection with D2 lymph node dissection for adenocarcinoma. Surg Endosc. 2008. 22:2753–2760.
Article14. Kim MC, Jung GJ, Kim HH. Learning curve of laparoscopy-assisted distal gastrectomy with systemic lymphadenectomy for early gastric cancer. World J Gastroenterol. 2005. 11:7508–7511.
Article15. Jin SH, Kim DY, Kim H, Jeong IH, Kim MW, Cho YK, et al. Multidimensional learning curve in laparoscopy-assisted gastrectomy for early gastric cancer. Surg Endosc. 2007. 21:28–33.
Article16. Park SS, Kim MC, Park MS, Hyung WJ. Rapid adaptation of robotic gastrectomy for gastric cancer by experienced laparoscopic surgeons. Surg Endosc. 2012. 26:60–67.
Article17. Song J, Kang WH, Oh SJ, Hyung WJ, Choi SH, Noh SH. Role of robotic gastrectomy using da Vinci system compared with laparoscopic gastrectomy: initial experience of 20 consecutive cases. Surg Endosc. 2009. 23:1204–1211.
Article18. Oh DK, Hur H, Kim JY, Han SU, Cho YK. V-shaped liver retraction during a laparoscopic gastrectomy for gastric cancer. J Gastric Cancer. 2010. 10:133–136.
Article19. Song HM, Lee SL, Hur H, Cho YK, Han SU. Linear-shaped gastroduodenostomy in totally laparoscopic distal gastrectomy. J Gastric Cancer. 2010. 10:69–74.
Article20. Hur H, Kim JY, Cho YK, Han SU. Technical feasibility of robot-sewn anastomosis in robotic surgery for gastric cancer. J Laparoendosc Adv Surg Tech A. 2010. 20:693–697.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Current status of robotic gastrectomy for gastric cancer: A review of recent randomized controlled trials
- Robotic surgery for gastric cancer
- Robotic Gastrectomy: The Current State of the Art
- Robotic Surgery for Early Gastric Cancer
- Robotic Roux-en-Y Gastric Bypass and Robotic Sleeve Gastrectomy for Morbid Obesity: Case Reports
