Long-Term Survival Following Port-Site Metastasectomy in a Patient with Laparoscopic Gastrectomy for Gastric Cancer: A Case Report
- Affiliations
-
- 1Department of Surgery, Yeouido St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. kimwook@catholic.ac.kr
- KMID: 2372207
- DOI: http://doi.org/10.5230/jgc.2015.15.3.209
Abstract
- A 78-year-old man underwent laparoscopy-assisted total gastrectomy for gastric cancer (pT3N0M0). Multiple port sites were used, including a 10 mm port for a videoscope at the umbilical point and three other working ports. During the six-month follow-up evaluation, a 2 cm enhancing mass confined to the muscle layer was found 12 mm from the right lower quadrant port site, suggesting a metastatic or desmoid tumor. Follow-up computed tomography imaging two months later showed that the mass had increased in size to 3.5 cm. We confirmed that there was no intra-abdominal metastasis by diagnostic laparoscopy and then performed a wide resection of the recurrent mass. The histologic findings revealed poorly differentiated adenocarcinoma, suggesting a metastatic mass from the stomach cancer. The postoperative course was uneventful, and the patient completed adjuvant chemotherapy with TS-1 (tegafur, gimeracil, and oteracil potassium). There was no evidence of tumor recurrence during the 50-month follow-up period.
Keyword
MeSH Terms
Figure
-
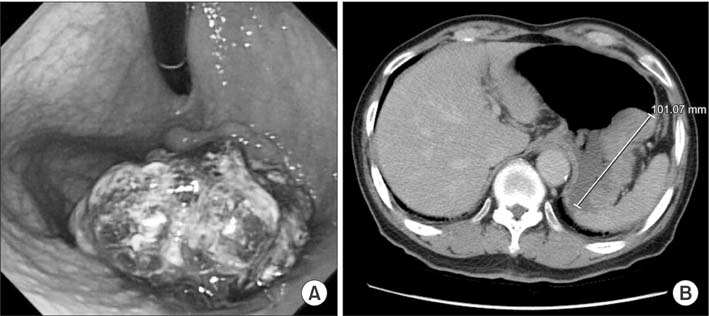
Fig. 1 (A) Gastrofiberscopy showing a large fungating mass at the fundus. (B) Computed tomography shows a 10 cm fungating mass without definite lymph node enlargement.

Fig. 2 Port placements for the laparoscopy-assisted total gastrectomy.
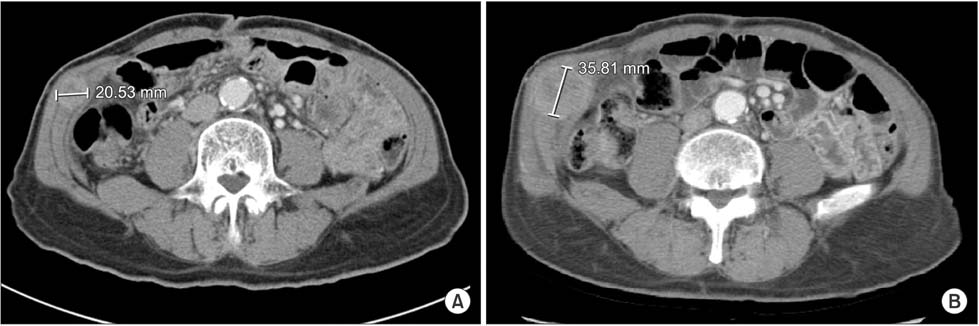
Fig. 3 (A) The follow-up computed tomography 6 months after surgery showed a 2 cm abdominal wall mass at the right lower quadrant port site. (B) The mass increased in size to nearly 3.5 cm during the 2-month observation period.
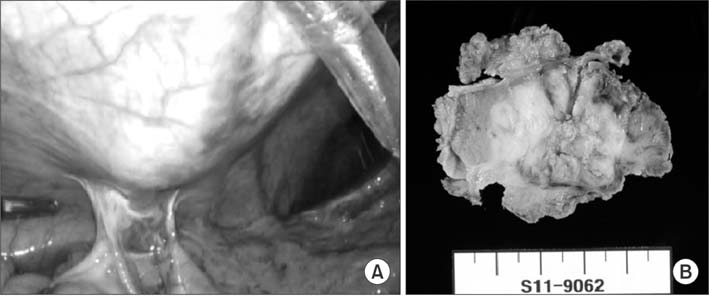
Fig. 4 (A) Diagnostic laparoscopy revealed no peritoneal metastasis or peritoneal invasion of the recurrent mass. (B) The metastasectomy specimen shows a 3.5×3.0 cm poorly defined white soft mass without invasion of the peritoneum.

Fig. 5 The histologic findings of the primary tumor (A) and abdominal wall tumor (B) were similar and suggested poorly differentiated adenocarcinoma in both samples (A, B: H&E, ×200).
Reference
-
1. Kim HH, Han SU, Kim MC, Hyung WJ, Kim W, Lee HJ, et al. Long-term results of laparoscopic gastrectomy for gastric cancer: a large-scale case-control and case-matched Korean multicenter study. J Clin Oncol. 2014; 32:627–633.2. Kim YW, Baik YH, Yun YH, Nam BH, Kim DH, Choi IJ, et al. Improved quality of life outcomes after laparoscopy-assisted distal gastrectomy for early gastric cancer: results of a prospective randomized clinical trial. Ann Surg. 2008; 248:721–727.3. Fang C, Hua J, Li J, Zhen J, Wang F, Zhao Q, et al. Comparison of long-term results between laparoscopy-assisted gastrectomy and open gastrectomy with D2 lymphadenectomy for advanced gastric cancer. Am J Surg. 2014; 208:391–396.4. Gordon AC, Kojima K, Inokuchi M, Kato K, Sugihara K. Long-term comparison of laparoscopy-assisted distal gastrectomy and open distal gastrectomy in advanced gastric cancer. Surg Endosc. 2013; 27:462–470.5. Jung YJ, Kim DJ, Lee JH, Kim W. Safety of intracorporeal circular stapling esophagojejunostomy using trans-orally inserted anvil (OrVil) following laparoscopic total or proximal gastrectomy: comparison with extracorporeal anastomosis. World J Surg Oncol. 2013; 11:209.6. Schaeff B, Paolucci V, Thomopoulos J. Port site recurrences after laparoscopic surgery. A review. Dig Surg. 1998; 15:124–134.7. Kazemier G, Bonjer HJ, Berends FJ, Lange JF. Port site metastases after laparoscopic colorectal surgery for cure of malignancy. Br J Surg. 1995; 82:1141–1142.8. Cava A, Román J, González Quintela A, Martín F, Aramburo P. Subcutaneous metastasis following laparoscopy in gastric adenocarcinoma. Eur J Surg Oncol. 1990; 16:63–67.9. Nduka CC, Monson JR, Menzies-Gow N, Darzi A. Abdominal wall metastases following laparoscopy. Br J Surg. 1994; 81:648–652.10. Rangarajan M. Multiple port-site and subcutaneous metastases following palliative laparoscopic surgery for advanced gastric cancer. Ann Acad Med Singapore. 2007; 36:875–876.11. Döbrönte Z, Wittmann T, Karácsony G. Rapid development of malignant metastases in the abdominal wall after laparoscopy. Endoscopy. 1978; 10:127–130.12. Stockdale AD, Pocock TJ. Abdominal wall metastasis following laparoscopy: a case report. Eur J Surg Oncol. 1985; 11:373–375.13. Sakurai K, Tanaka H, Lee T, Muguruma K, Kubo N, Yashiro M, et al. Port site metastasis after laparoscopic-assisted distal gastrectomy (LADG). Int Surg. 2013; 98:363–366.14. Hwang SI, Kim HO, Yoo CH, Shin JH, Son BH. Laparoscopic-assisted distal gastrectomy versus open distal gastrectomy for advanced gastric cancer. Surg Endosc. 2009; 23:1252–1258.15. Jeong SH, Lee YJ, Park ST, Choi SK, Hong SC, Jung EJ, et al. Risk of recurrence after laparoscopy-assisted radical gastrectomy for gastric cancer performed by a single surgeon. Surg Endosc. 2011; 25:872–878.16. Lee YJ, Ha WS, Park ST, Choi SK, Hong SC. Port-site recurrence after laparoscopy-assisted gastrectomy: report of the first case. J Laparoendosc Adv Surg Tech A. 2007; 17:455–457.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Role of Metastasectomy on Overall Survival of Patients with Metastatic Gastric Cancer
- Single-Port Laparoscopic Proximal Gastrectomy with Double Tract Reconstruction for Early Gastric Cancer: Report of a Case
- Single Port Gastrectomy for Gastric Cancer
- Long-Term Oncological Outcomes of Reduced Three-Port Laparoscopic Gastrectomy for Early-Stage Gastric Carcinoma: a Retrospective Large-Scale Multi-Institutional Study
- Robotic Gastrectomy for Gastric Cancer: A Review of Postoperative and Oncologic Outcomes
