Ann Dermatol.
2017 Feb;29(1):91-94. 10.5021/ad.2017.29.1.91.
Almost Unilateral Focal Dermal Hypoplasia
- Affiliations
-
- 1Department of Dermatology, Wonju Severance Christian Hospital, Yonsei University Wonju College of Medicine, Wonju, Korea. ahnsk@yonsei.ac.kr
- KMID: 2368035
- DOI: http://doi.org/10.5021/ad.2017.29.1.91
Abstract
- Focal dermal hypoplasia, caused by mutations in PORCN, is an X-linked ectodermal dysplasia, also known as Goltz syndrome. Only seven cases of unilateral or almost unilateral focal dermal hypoplasia have been reported in the English literature and there have been no previously reported cases in the Republic of Korea. A 19-year-old female presented with scalp defects, skin lesions on the right leg and the right trunk, and syndactyly of the right fourth and fifth toes. Cutaneous examination revealed multiple atrophic plaques and a brown and yellow mass with fat herniation and telangiectasia that was mostly located on the lower right leg. She had syndactyly on the right foot and the scalp lesion appeared to be an atrophic, membranous, fibrotic alopecic scar. A biopsy of the calf revealed upper dermal extension of fat cells, dermal atrophy, and loss of dermal collagen. A diagnosis of almost unilateral focal dermal hypoplasia was made on the basis of physical and histologic findings. Henceforth, the patient was referred to a plastic surgeon and an orthopedics department to repair her syndactyly.
MeSH Terms
Figure
-
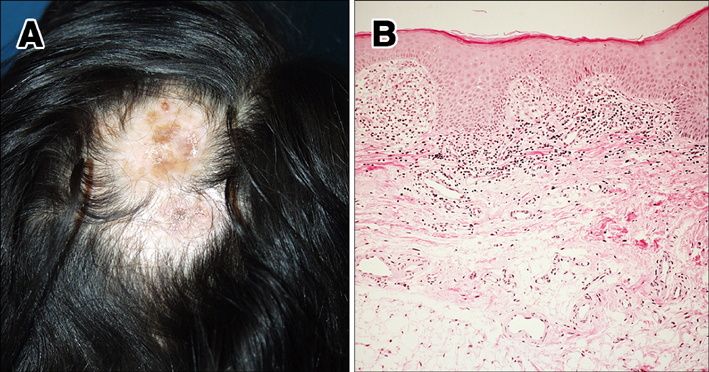
Fig. 1 (A) Atrophic and fibrotic alopecic patch on the scalp. (B) Irregularly thickened epidermis and atrophic dermis with upward extending subcutaneous tissue. Mild fibrotic change and loss of periadnexal structures (H&E, ×40).

Fig. 2 (A) Irregular shaped large atrophic patch with telangiectasia on the right side of the abdomen. (B) Multiple and various sized protruding yellowish masses and atrophic patches mostly on the right side of the leg. Only some of linear streaks are seen on the left side (inset: protruding mass with fat herniation and deposition). (C) Syndactyly of the fourth and fifth toes on the right root.
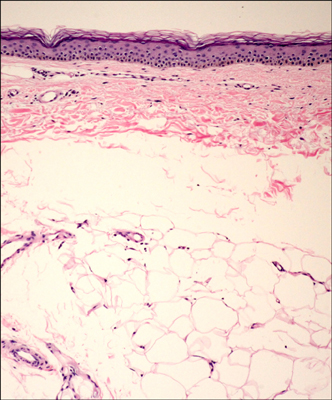
Fig. 3 Marked thinning of the dermis and extension of subcutaneous fat toward the epidermis (H&E, ×40).
Reference
-
1. Goltz RW, Peterson WC, Gorlin RJ, Ravits HG. Focal dermal hypoplasia. Arch Dermatol. 1962; 86:708–717.
Article2. Goltz RW, Henderson RR, Hitch JM, Ott JE. Focal dermal hypoplasia syndrome. A review of the literature and report of two cases. Arch Dermatol. 1970; 101:1–11.
Article3. Adaimy L, Chouery E, Megarbane H, Mroueh S, Delague V, Nicolas E, et al. Mutation in WNT10A is associated with an autosomal recessive ectodermal dysplasia: the odonto-onycho-dermal dysplasia. Am J Hum Genet. 2007; 81:821–828.
Article4. Grzeschik KH, Bornholdt D, Oeffner F, König A, del Carmen Boente M, Enders H, et al. Deficiency of PORCN, a regulator of Wnt signaling, is associated with focal dermal hypoplasia. Nat Genet. 2007; 39:833–835.
Article5. Wang X, Reid Sutton V, Omar Peraza-Llanes J, Yu Z, Rosetta R, Kou YC, et al. Mutations in X-linked PORCN, a putative regulator of Wnt signaling, cause focal dermal hypoplasia. Nat Genet. 2007; 39:836–838.
Article6. Grigoryan T, Wend P, Klaus A, Birchmeier W. Deciphering the function of canonical Wnt signals in development and disease: conditional loss- and gain-of-function mutations of beta-catenin in mice. Genes Dev. 2008; 22:2308–2341.
Article7. Bae YI, Yun SJ, Lee JB, Kim SJ, Won YH, Lee SC. A case of goltz syndrome. Korean J Dermatol. 2008; 46:122–125.8. Frieden IJ. Aplasia cutis congenita: a clinical review and proposal for classification. J Am Acad Dermatol. 1986; 14:646–660.
Article9. Stalder JF, Delaire J, David A, Cohen JY, Le Pape A. Unilateral Goltz syndrome in a boy. Ann Dermatol Venereol. 1984; 111:829–830.10. Denis-Thely L, Cordier MP, Cambazard F, Misery L. Unilateral focal dermal hypoplasia. Ann Dermatol Venereol. 2002; 129:1161–1163.11. Aoyama M, Sawada H, Shintani Y, Isomura I, Morita A. Case of unilateral focal dermal hypoplasia (Goltz syndrome). J Dermatol. 2008; 35:33–35.
Article12. Fernández-Torres R, Del Pozo J, García-Silva J, Fonseca E. Unilateral focal dermal hypoplasia. Actas Dermosifiliogr. 2010; 101:96–98.
Article13. Tenkir A, Teshome S. Goltz syndrome (focal dermal hypoplasia) with unilateral ocular, cutaneous and skeletal features: case report. BMC Ophthalmol. 2010; 10:28.
Article14. Maalouf D, Mégarbané H, Chouery E, Nasr J, Badens C, Lacoste C, et al. A novel mutation in the PORCN gene underlying a case of almost unilateral focal dermal hypoplasia. Arch Dermatol. 2012; 148:85–88.
Article15. Asano M, Fujimura T, Wakusawa C, Aoki Y, Matsubara Y, Aiba S. A case of almost unilateral focal dermal hypoplasia resulting from a novel mutation in the PORCN gene. Acta Derm Venereol. 2013; 93:120–121.
Article16. Alster TS, Wilson F. Focal dermal hypoplasia (Goltz's syndrome). Treatment of cutaneous lesions with the 585-nm flashlamp-pumped pulsed dye laser. Arch Dermatol. 1995; 131:143–144.
Article
