Early and Midterm Results Following Interventional Coarctoplasty: Evaluation of Variables that Can Affect the Results
- Affiliations
-
- 1Cardiovascular Intervention Research Center, Rajaie Cardiovascular Medical and Research Center, Iran University of Medical Sciences, Tehran, Iran. safeabdi@gmail.com
- KMID: 2365288
- DOI: http://doi.org/10.4070/kcj.2016.0211
Abstract
- BACKGROUND AND OBJECTIVES
Stent coarctoplasty has been approved as the treatment of choice for adult patients with coarctation of the aorta. We have evaluated the early and midterm clinical and procedural results after interventional coarctoplasty. Also, variables that can affect these results were evaluated.
SUBJECTS AND METHODS
Gathering clinical, angiographic and procedural data, we evaluated the pre-specified outcomes, including procedural success, complications, the incidence of hypertension after coarctoplasty etc., after the procedure. The effect of pre-specified variables including aortic arch shape, coarctation type and etc. on the procedural result was evaluated.
RESULTS
Between February 2005 through March 2014, 133 stent coarctoplasty procedures were performed. Median age was 23.5 years old (interquartile range [IQR]:19-28), and 105 (71.9%) were male. Nearly all of the patients were undergone stent coarctoplasty, mostly with cheatham platinum (CP) stents. There was no association between aortic arch morphology and acute procedural complications. Balloon length more than 40 mm (p=0.028), aorta diameter at the site of Coarctation larger than 2.35 mm (p=0.008) was associated with higher rate of restenosis during follow-up. Comparison between the prevalence of hypertension (HTN) before and after coarctoplasty showed a significant reduction in the prevalence of HTN (117 [91.4%] vs. 95 [74.2%] p<0.001).
CONCLUSION
Stent coarctoplasty is a low-risk procedure with favorable early and delayed outcomes. Most mortality is related to the patient's comorbid conditions and not to the procedure.
Keyword
MeSH Terms
Figure
-

Fig. 1 Anatomical variants of the aortic arch. (A) The width and height of arch are nearly equal; it is typical for Circular arch. (B) The width is shorter than height in the typical Gothic arch. (C) Crenel arch is defined by shorter height than width. The picture beneath description of juxta and postductal coarctation. The distance between SCA origin to the coarctation site narrowing is the reference for such definition. In this case, the length is about 16 mm, which is categorized as postductal. Note the presence of localized dissection at the coarctation site with involvement of SCA origin and arch. The dissection occurred during wiring of coarctation. The covered stent was used for this patient because of dissection. SCA: subclavian artery.
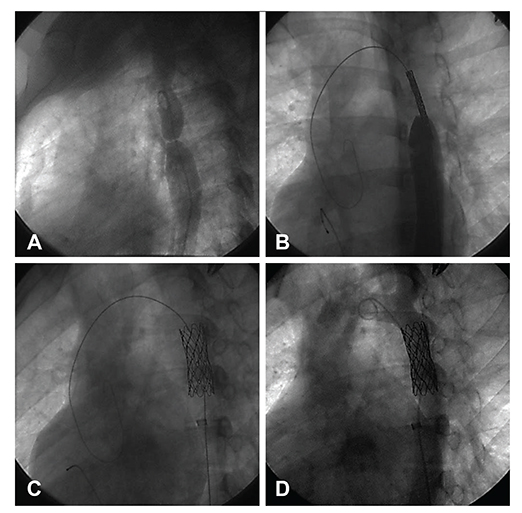
Fig. 2 Stent coarctoplasty. (A) Injection of the contrast media at descending aorta after passing the pigtail catheter over a 0.035 inch-wire. (B) Positioning of the stent. (C) Stent deployment during rapid pacing. (D) Final result.

Fig. 3 Management of a patient with aortic perforation after stent deployment. (A, B) After the stent was deployed at the site of this postductal coarctation, contrast injection revealed a tiny but important contrast leakage at the distal edge of the stent. (C) A CP 38 covered stent deployed to cover the perforation site, but the leakage persisted. (D, E) Post dilation causes the leakage to stop. CP: cheatham platinum.
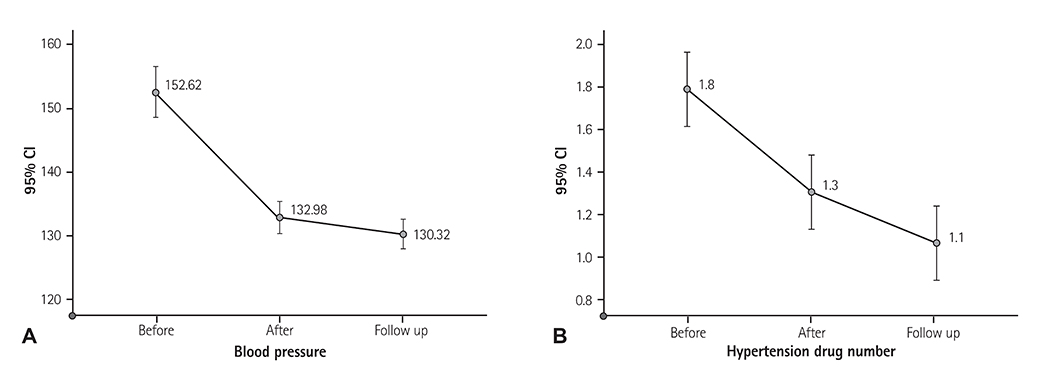
Fig. 4 Reduction in blood pressure and antihypertensive drugs number pattern after treatment of the coarctation of the aorta. (A) Systolic BP and (B) number of drugs were used for treating HTN, just after coarctoplasty and at the end of follow-up. CI: confidence interval, BP: blood pressure, HTN: hypertension.
Reference
-
1. Peters B, Ewert P, Berger F. The role of stents in the treatment of congenital heart disease: current status and future perspectives. Ann Pediatr Cardiol. 2009; 2:3–23.2. Baykan A, Karaqoz T, Celiker A. Endovascular stent implantation for coarctation of the aorta in children and young adults. Immediately follow-up results from Turkey. Turk J Pediatr. 2009; 51:116–119.3. Godart F. Intravascular stenting for the treatment of coarctation of the aorta in adolescent and adult patients. Arch Cardiovasc Dis. 2011; 104:627–635.4. Marshall AC, Perry SB, Keane JF, et al. Early results and medium-term follow-up of stent implantation for residual or recurrent aortic coarctation. Am Heart J. 2000; 139:1054–1060.5. Holzer R, Qureshi S, Ghasemi A, Lock JE. Stenting of aortic coarctation: acute, intermediate, and long-term results of a prospective multi-institutional registry-Congenital Cardiovascular Interventional Study Consortium (CCISC). Catheter Cardiovasc Interv. 2010; 76:553–563.6. Felts TF, Bacha E, Beekman RH 3rd, et al. Indications for cardiac catheterization and intervention in pediatric cardiac disease: a scientific statement from the American Heart Association. Circulation. 2011; 123:2607–2652.7. Ringel RE, Gauvreau K, Moses H, Jenkins KJ. Coarctation of the aorta stent trial (COAST): study design and rationale. Am Heart J. 2012; 164:7–13.8. Ou P, Mousseaux E, Celermajer DS, et al. Aortic arch shape deformation after coarctation surgery: effect on blood pressure response. J Thorac Cardiovasc Surg. 2006; 132:1105–1111.9. Forbes TJ, Garekar S, Amin Z, et al. Procedural results and acute complications in stenting native and recurrent coarctation of the aorta in patients over 4 years of age: a multi-institutional study. Catheter Cardiovasc Interv. 2007; 70:276–285.10. McCrindle BW, Jones TK, Morrow WR, et al. Acute results of balloon angioplasty of native coarctation versus recurrent aortic obstruction are equivalent. Valvuloplasty and Angioplasty of Congenital Anomalies (VACA) registry investigators. J Am Coll Cardiol. 1996; 28:1810–1817.11. Forbes TJ, Kim DW, Du W, et al. Comparison of surgical, stent, and balloon angioplasty treatment of native coarctation of the aorta: an observational study by the CCISC (Congenital Cardiovascular Interventional Study Consortium). J Am Coll Cardiol. 2011; 58:2664–2674.12. Harrison DA, McLaughlin PR, Lazzam C, Connelly M, Benson LN. Endovascular stents in the management of coarctation of the aorta in the adolescent and adult: one year follow up. Heart. 2001; 85:561–566.13. Mullen MJ. Coarctation of the aorta in adults: do we need surgeons? Heart. 2003; 89:3–5.14. Turner DR, Gaines PA. Endovascular management of coarctation of the aorta. Semin Intervent Radiol. 2007; 24:153–166.15. Forbes TJ, Moore P, Pedra CA, et al. Intermediate follow-up following intravascular stenting for treatment of coarctation of the aorta. Catheter Cardiovasc Interv. 2007; 70:569–577.16. Chen SS, Donald AE, Storry C, Halcox JP, Bonhoeffer P, Deanfield JE. Impact of aortic stenting on peripheral vascular function and daytime systolic blood pressure in adult coarctation. Heart. 2008; 94:919–924.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Unpredictable Midterm Coronary Damage after Knuckle-reverse CART: Should We Be More Careful?
- Evaluation of Resting Blood Pressures, Left Ventricular Function and Mass in Young Children with Successful Coarctoplasty in Infancy
- Influences of Affect States and Mood Congruent/Incongruent Variables on Psychosis-Proneness
- The Relationship between Senior Year Examinations at a Medical School and the Korean Medical Licensing Examination
- Comparative Analysis of Structural, Process, and Outcome Indicators for Evaluating the Quality of Nursing Care
