Multi-Detector CT Coronary Angiographic Findings of Coronary-to-Pulmonary Artery Fistula
- Affiliations
-
- 1Department of Radiology, Seoul National University Hospital, Seoul, Korea. iameuna1@gmail.com
- 2Department of Radiology, Myongji Hospital, Seonam University College of Medicine, Goyang, Korea.
- KMID: 2365050
- DOI: http://doi.org/10.3348/jksr.2017.76.1.39
Abstract
- PURPOSE
To evaluate multi-detector CT (MDCT) coronary angiographic findings of coronary-to-pulmonary artery fistula (CPAF).
MATERIALS AND METHODS
We retrospectively reviewed images of patients with CPAF from the coronary CT angiography (CCTA) database obtained with a 64-channel MDCT between January 2008 and March 2011. We analyzed the CCTA findings for feeding arteries, fistula, association with peripulmonary arterial aneurysms, and the presence of communication between the CPAF and bronchial arteries.
RESULTS
Fifty-five of the 15042 (0.37%) patients were diagnosed with CPAFs. The feeding artery was single (n = 18) or multiple (n = 37). The fistula had a single drainage site (n = 54) or multiple drainage sites (n = 1). The mean diameter of the fistulous opening was 2.7 ± 1.4 mm. A peripulmonary arterial aneurysm was present in 24 (44%) patients. Communication between CPAF and bronchial arteries was present in eight (14.5%) patients.
CONCLUSION
MDCT coronary angiography can provide comprehensive morphologic details on CPAF and may help in presurgical or preinterventional planning.
MeSH Terms
Figure
-
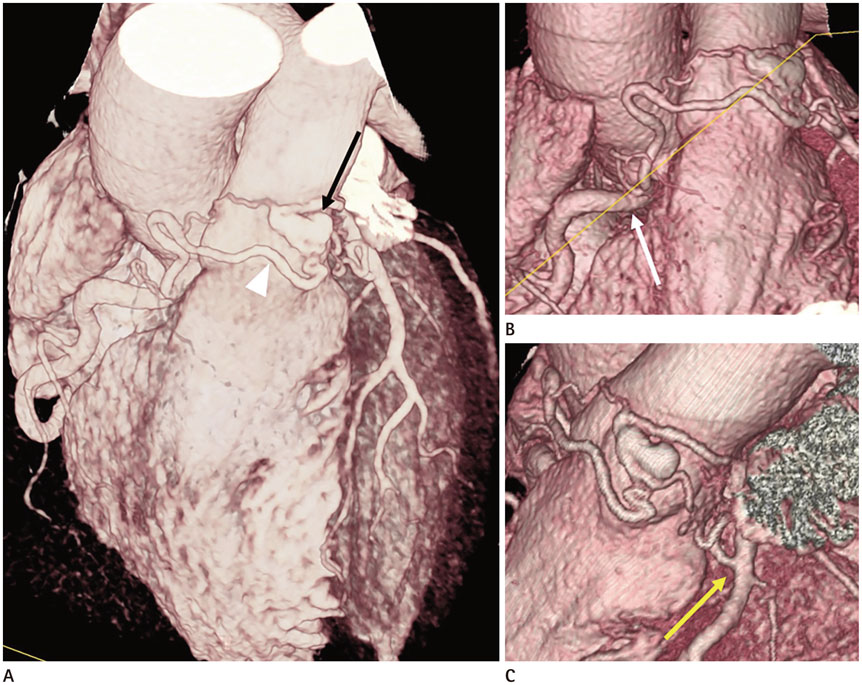
Fig. 1 Coronary-to-pulmonary artery fistula (CPAF) with multiple feeding arteries in a 59-year-old man. A. The tortuous vessels of CPAF (arrowhead) pass anterior to the pulmonary artery, forming a network and focal aneurysmal sac (black arrow) before they enter the main pulmonary artery. B, C. The multiple feeding arteries of the CPAF arise from (B) the right coronary artery (white arrow) and (C) the proximal left anterior descending artery (yellow arrow).
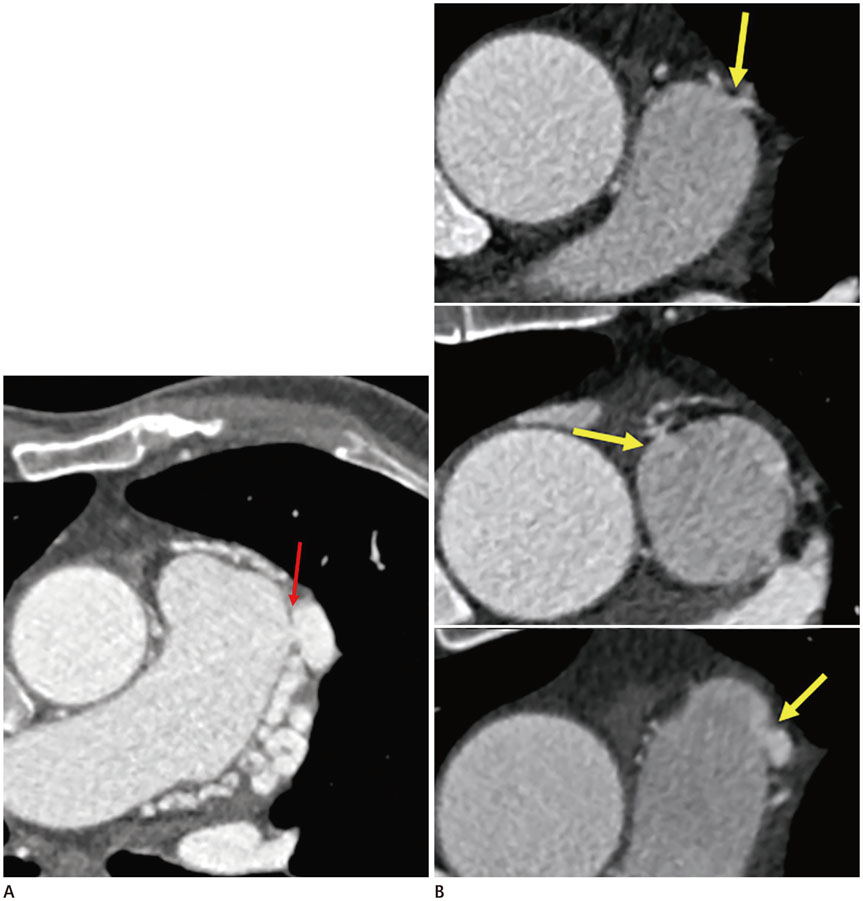
Fig. 2 Drainage sites of coronary-to-pulmonary artery fistulae (CPAFs). A. A case of a 63-year-old man. The single drainage site is located in the left sinus of the main pulmonary artery (red arrow). B. A case of a 70-year-old man. The CPAF drained into three different points in the left and right sinuses of the main pulmonary artery (yellow arrows).
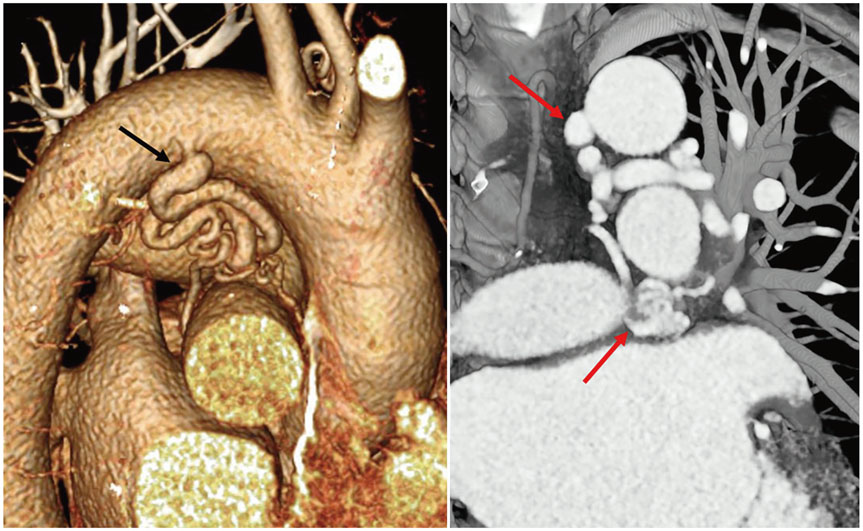
Fig. 3 Coronary-to-pulmonary artery fistula (CPAF) communicating with bronchial arteries in a 63-year-old man. The bronchial artery originates from the proximal descending thoracic aorta (black arrow). It runs under the left pulmonary artery (red arrows) and communicates with the abnormal serpentine vessels that lead to the formation of CPAF.
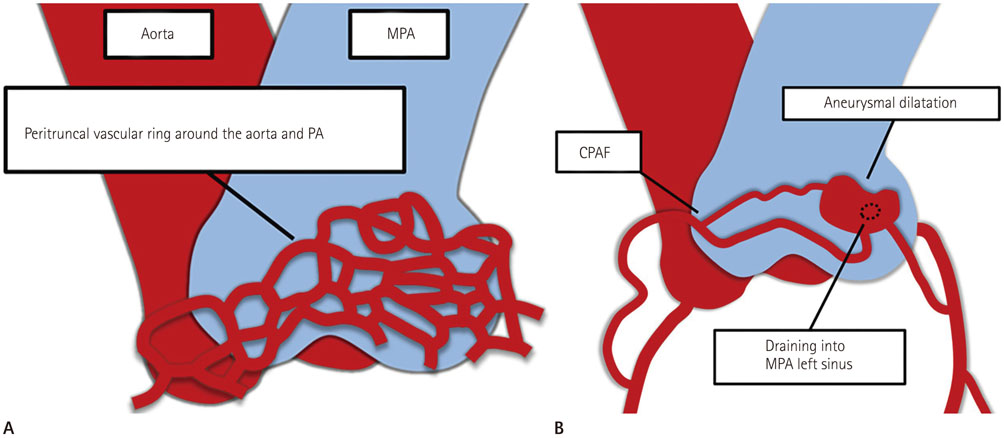
Fig. 4 Development of coronary-to-pulmonary artery fistula (CPAF), illustrated based on references (910). A. Peritruncal vascular network formation around the primitive aorta and pulmonary artery. B. Development of CPAF as a result of abnormal vasculogenesis in the left sinus of the main pulmonary artery (MPA) with accompanying aneurysmal dilatation.
Cited by 1 articles
-
Coronary-to-Pulmonary Artery Fistula in Adults: Natural History and Management Strategies
Hokun Kim, Kyongmin Sarah Beck, Yeon Hyeon Choe, Jung Im Jung
Korean J Radiol. 2019;20(11):1491-1497. doi: 10.3348/kjr.2019.0331.
Reference
-
1. Demirelli S, Tas MH, Simsek Z, Duman H, Ipek E. Coronaryto-pulmonary artery fistula and concomitant acute coronary syndrome: two cases. J Case Rep. 2014; 4:56–59.2. Vaidyanathan KR, Theodore SA, Sankar MN, Cherian KM. Coronary artery to pulmonary artery fistula with dual origin--embryological, clinical and surgical significance. Eur J Cardiothorac Surg. 2007; 31:318–319.3. Gandy KL, Rebeiz AG, Wang A, Jaggers JJ. Left main coronary artery-to-pulmonary artery fistula with severe aneurysmal dilatation. Ann Thorac Surg. 2004; 77:1081–1083.4. Vanhoenacker PK, Heijenbrok-Kal MH, Van Heste R, Decramer I, Van Hoe LR, Wijns W, et al. Diagnostic performance of multidetector CT angiography for assessment of coronary artery disease: meta-analysis. Radiology. 2007; 244:419–428.5. Dodd JD, Ferencik M, Liberthson RR, Cury RC, Hoffmann U, Brady TJ, et al. Congenital anomalies of coronary artery origin in adults: 64-MDCT appearance. AJR Am J Roentgenol. 2007; 188:W138–W146.6. Haller S, Kaiser C, Buser P, Bongartz G, Bremerich J. Coronary artery imaging with contrast-enhanced MDCT: extracardiac findings. AJR Am J Roentgenol. 2006; 187:105–110.7. Ohkura K, Yamashita K, Terada H, Washiyama N, Akuzawa S. Congenital systemic and coronary-to-pulmonary artery fistulas. Ann Thorac Cardiovasc Surg. 2010; 16:203–206.8. Takx RA, Suchá D, Park J, Leiner T, Hoffmann U. Sublingual nitroglycerin administration in coronary computed tomography angiography: a systematic review. Eur Radiol. 2015; 25:3536–3542.9. Park EA, Lee W, Na SH, Chung JW, Park JH. Left ventricular fat deposition on CT in patients without proven myocardial disease. Int J Cardiovasc Imaging. 2013; 29:Suppl 1. 37–45.10. de Oliveira, da Silva, Mandarimde-Lacerda CA. Origin and development of the coronary arteries. Int J Morphol. 2009; 27:891–898.11. Kazuno K, Akasaka N, Kiyokawa K, Sasajima T. Ruptured aneurysm of coronary artery-to-pulmonary artery fistula. Asian Cardiovasc Thorac Ann. 2012; 20:324–326.12. Chang DS, Lee MH, Lee HY, Barack BM. MDCT of left anterior descending coronary artery to main pulmonary artery fistula. AJR Am J Roentgenol. 2005; 185:1258–1260.13. Angelini P. Coronary-to-pulmonary fistulae: what are they? What are their causes? What are their functional consequences? Tex Heart Inst J. 2000; 27:327–329.14. Said SA, Landman GH. Coronary-pulmonary fistula: long-term follow-up in operated and non-operated patients. Int J Cardiol. 1990; 27:203–210.15. Urrutia-S CO, Falaschi G, Ott DA, Cooley DA. Surgical management of 56 patients with congenital coronary artery fistulas. Ann Thorac Surg. 1983; 35:300–307.16. Kim MS, Jung JI, Chun HJ. Coronary to pulmonary artery fistula: morphologic features at multidetector CT. Int J Cardiovasc Imaging. 2010; 26:Suppl 2. 273–280.17. Lim JJ, Jung JI, Lee BY, Lee HG. Prevalence and types of coronary artery fistulas detected with coronary CT angiography. AJR Am J Roentgenol. 2014; 203:W237–W243.18. Saboo SS, Juan YH, Khandelwal A, George E, Steigner ML, Landzberg M, et al. MDCT of congenital coronary artery fistulas. AJR Am J Roentgenol. 2014; 203:W244–W252.19. Zhang LJ, Zhou CS, Wang Y, Jin Z, Yu W, Zhang Z, et al. Prevalence and types of coronary to pulmonary artery fistula in a Chinese population at dual-source CT coronary angiography. Acta Radiol. 2014; 55:1031–1039.20. Erol C, Seker M. Coronary artery anomalies: the prevalence of origination, course, and termination anomalies of coronary arteries detected by 64-detector computed tomography coronary angiography. J Comput Assist Tomogr. 2011; 35:618–624.21. Hoendermis ES, Waterbolk TW, Willems TP, Zijlstra F. Large common left and right coronary artery to coronary sinus fistula. Interact Cardiovasc Thorac Surg. 2006; 5:788–789.22. van Geuns RJM, Cademartiri F. Anatomy of the coronary arteries and veins in CT imaging. In : Schoepf UJ, editor. CT of the Heart. Totowa, NJ: Humana Press;2005. p. 219–227. .23. Gowda RM, Vasavada BC, Khan IA. Coronary artery fistulas: clinical and therapeutic considerations. Int J Cardiol. 2006; 107:7–10.24. Shabestari AA, Akhlaghpoor S, Fatehi M. Findings of bilateral coronary to pulmonary artery fistula in 64-multislice computed tomographic angiography: correlation with catheter angiography. J Comput Assist Tomogr. 2008; 32:271–273.25. Shriki JE, Shinbane JS, Rashid MA, Hindoyan A, Withey JG, DeFrance A, et al. Identifying, characterizing, and classifying congenital anomalies of the coronary arteries. Radiographics. 2012; 32:453–468.26. Rittenhouse EA, Doty DB, Ehrenhaft JL. Congenital coronary artery- cardiac chamber fistula. Review of operative management. Ann Thorac Surg. 1975; 20:468–485.27. Tomasian A, Lell M, Currier J, Rahman J, Krishnam MS. Coronary artery to pulmonary artery fistulae with multiple aneurysms: radiological features on dual-source 64-slice CT angiography. Br J Radiol. 2008; 81:e218–e220.28. Lai MC, Chen WJ, Chiang CW, Ko YL. An unusual case of dual coronary artery fistulas to main pulmonary artery. Chang Gung Med J. 2002; 25:51–55.29. Härle T, Kronberg K, Elsässer A. Coronary artery fistula with myocardial infarction due to steal syndrome. Clin Res Cardiol. 2012; 101:313–315.30. Qiu MJ, Dong DJ. Myocardial infarction following bronchial artery embolization for hemoptysis. Chin Med J (Engl). 2013; 126:997.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Unusual Coronary Artery Fistula: Left Anterior Descending Coronary Artery - Left Ventricular Fistula Diagnosed by ECG-Gated Multi-Detector Row Coronary CT Angiography
- A Case of Coronary Arteriovenous Fistula Associated with Pulmonary Artery Aneurysm Confirmed by Multi Detector-Row Helical CT
- A case of coronary artery-pulmonary artery fistula communicated with aorto-pulmonary fistula via common channel detected by Multidetector row CT (MDCT) and coronary angiography
- Left Circumflex Coronary Artery Fistula Connected to the Right Bronchial Artery Associated with Bronchiectasis: Multidetector CT and Coronary Angiography Findings
- Complex Coronary Cameral Fistulas Evaluated by Multi-Detector CT Angiography: A Report of Three Rare Cases and a Review of the Literature
