Clinical Usefulness of Bronchoalveolar Lavage Cellular Analysis and Lymphocyte Subsets in Diffuse Interstitial Lung Diseases
- Affiliations
-
- 1Department of Laboratory Medicine, Ewha Womans University School of Medicine, Seoul, Korea. JungWonH@ewha.ac.kr
- KMID: 2363182
- DOI: http://doi.org/10.3343/alm.2015.35.2.220
Abstract
- BACKGROUND
Diffuse interstitial lung diseases (DILDs) form a part of a heterogeneous group of respiratory diseases. Bronchoalveolar lavage (BAL) analysis has been used for differential diagnosis of DILDs, but their clinical usefulness is controversial. The aim of this study was to investigate the clinical usefulness of BAL cellular analysis with lymphocyte subsets for the differential diagnosis of DILDs.
METHODS
A total of 69 patients diagnosed with DILDs were enrolled. Basic demographic data, BAL cellular analysis with lymphocyte subsets, histology, and high resolution computed tomogram (HRCT) findings were analyzed and compared as per disease subgroup.
RESULTS
Significant differences were found between groups in the proportion of neutrophils (P=0.0178), eosinophils (P=0.0003), T cells (P=0.0305), CD4 cells (P=0.0002), CD8 cells (P<0.0001), and CD4/CD8 ratio (P<0.0001). These findings were characteristic features of eosinophilic pneumonia and sarcoidosis. Other parameters were not significantly different between groups. At the cut-off value of 2.16 for sarcoidosis, CD4/CD8 ratio showed sensitivity of 91.7% (95% CI, 61.5-98.6%) and specificity of 84.2% (95% CI, 72.1-92.5%).
CONCLUSIONS
Routine analysis of BAL lymphocyte subset may not provide any additional benefit for differential diagnosis of DILDs, except for conditions where BAL is specifically indicated, such as eosinophilic pneumonia or sarcoidosis.
Keyword
MeSH Terms
-
Aged
Aged, 80 and over
Area Under Curve
Bronchoalveolar Lavage Fluid/*cytology
CD4-CD8 Ratio
Demography
Eosinophils/cytology
Female
Humans
Immunophenotyping
Lung Diseases, Interstitial/*diagnosis/diagnostic imaging
Lymphocyte Subsets/*cytology
Male
Middle Aged
Neutrophils/cytology
ROC Curve
Sarcoidosis/diagnosis
T-Lymphocytes/cytology
Tomography, X-Ray Computed
Figure
-
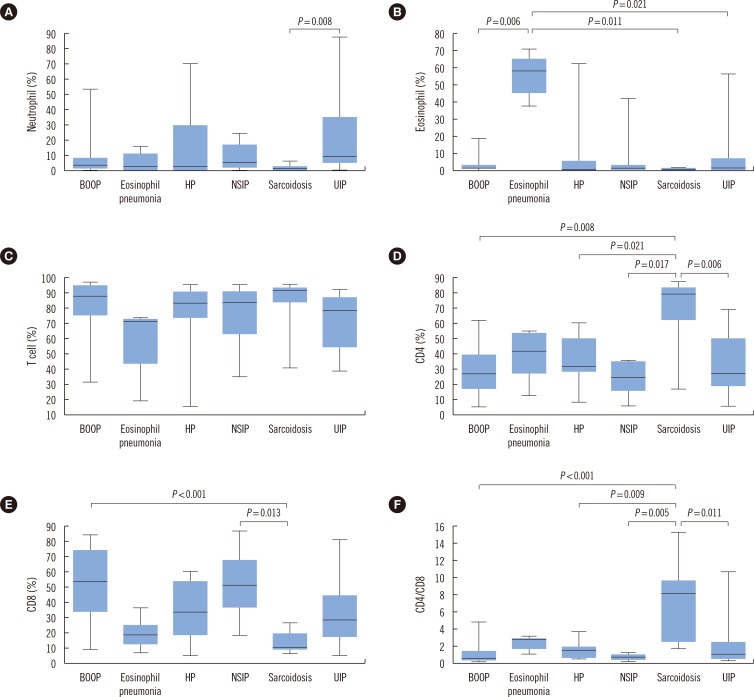
Fig. 1 Post-hoc analysis of parameters between groups. (A) Neutrophil, (B) Eosinophil, (C) T cell, (D) CD4 cell, (E) CD8 cell, and (F) CD4/CD8 ratio. Post-hoc analysis between groups and statistical significance are shown. Eosinophil % showed a significant difference in the eosinophilic pneumonia group and CD4 cell %, CD8 cell %, and CD4/CD8 ratio in the sarcoidosis group.Abbreviations: See Table 1.
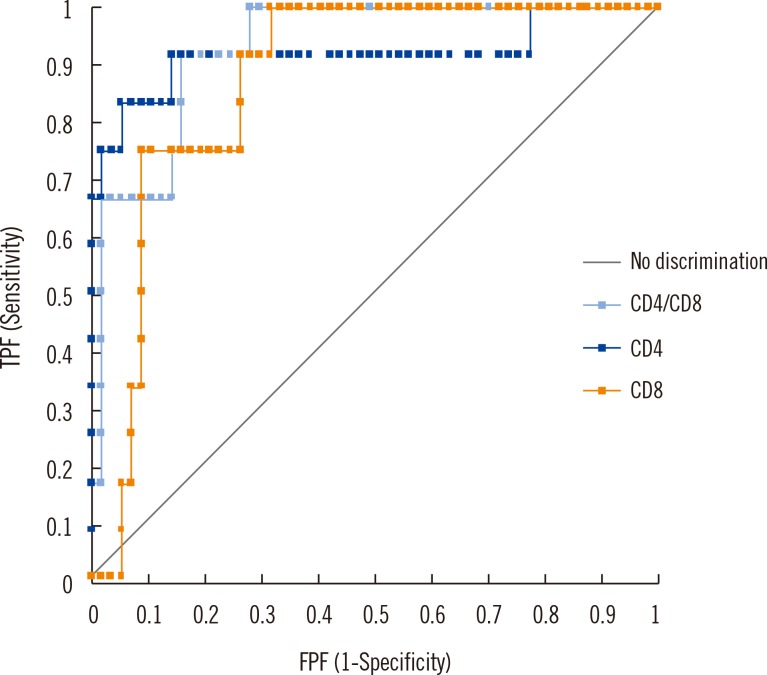
Fig. 2 Comparison of ROC curve for sarcoidosis (CD4, CD8, and CD4/CD8). The ROC curve for sarcoidosis diagnosis shows that the area under curve (AUC) was 0.918, 0.873, and 0.930 for CD4 cell %, CD8 cell %, and CD4/CD8 ratio, respectively, but no statistical difference was found among the variables (P>0.13). Based on the Youden index, cut-off of CD4/CD8 ratio for sarcoidosis was determined at 2.16, with sensitivity of 91.7% (95% CI, 61.5-98.6%) and specificity of 84.2% (95% CI, 72.1-92.5%).Abbreviations: TPF, true positive fraction; FPF, false positive fraction.
Reference
-
1. Kim DS. Diagnostic approaches to diffuse interstitial lung diseases. J Korean Med Assoc. 2009; 52:5–13.
Article2. Meyer KC, Raghu G, Baughman RP, Brown KK, Costabel U, du Bois RM, et al. An official American Thoracic Society clinical practice guideline: the clinical utility of bronchoalveolar lavage cellular analysis in interstitial lung disease. Am J Respir Crit Care Med. 2012; 185:1004–1014. PMID: 22550210.
Article3. Song KS, Heo WB, Won DI. Comparative analysis of bronchoalveolar lavages in interstitial lung diseases. Korean J Lab Med. 2007; 27:221–227. PMID: 18094580.
Article4. Jara-Palomares L, Martín-Juan J, Gómez-Izquierdo L, Cayuela-Domínguez A, Rodríguez-Becerra E, Rodríguez-Panadero F. Bronchoalveolar lavage findings in patients with diffuse interstitial lung disease: prospective study of a cohort of 562 patients. Arch Bronconeumol. 2009; 45:111–117. PMID: 19286112.
Article5. Ryu YJ, Chung MP, Han J, Kim TS, Lee KS, Chun EM, et al. Bronchoalveolar lavage in fibrotic idiopathic interstitial pneumonias. Respir Med. 2007; 101:655–660. PMID: 16919929.6. Technical recommendations and guidelines for bronchoalveolar lavage (BAL). Report of the European Society of Pneumology Task Group. Eur Respir J. 1989; 2:561–585. PMID: 2663535.7. Costabel U, Donner CF, Haslam PL, Rizzato G, Teschler H, Velluti G, et al. Clinical guidelines and indications for bronchoalveolar lavage (BAL): occupational lung diseases due to inhalation of inorganic dust. Eur Respir J. 1990; 3:946–949. 961–969. PMID: 2292297.8. Clinical guidelines and indications for bronchoalveolar lavage (BAL): Report of the European Society of Pneumology Task Group on BAL. Eur Respir J. 1990; 3:937–976. PMID: 2292291.9. Haslam PL, Baughman RP. Report of ERS Task Force: guidelines for measurement of acellular components and standardization of BAL. Eur Respir J. 1999; 14:245–248. PMID: 10515395.
Article10. The BAL Cooperative Group Streering Committee. Bronchoalveolar lavage constituents in healthy individuals, idiopathic pulmonary fibrosis, and selected comparison groups. Am Rev Respir Dis. 1990; 141:S169–S202. PMID: 2186681.11. Veeraraghavan S, Latsi PI, Wells AU, Pantelidis P, Nicholson AG, Colby TV, et al. BAL findings in idiopathic nonspecific interstitial pneumonia and usual interstitial pneumonia. Eur Respir J. 2003; 22:239–244. PMID: 12952254.
Article12. Wells AU. The clinical utility of bronchoalveolar lavage in diffuse parenchymal lung disease. Eur Respir Rev. 2010; 19:237–241. PMID: 20956199.
Article13. Meyer KC, Raghu G. Bronchoalveolar lavage for the evaluation of interstitial lung disease: is it clinically useful? Eur Respir J. 2011; 38:761–769. PMID: 21540304.
Article14. Meyer KC. The clinical utility of bronchoalveolar lavage in interstitial lung disease-is it really useful? Expert Rev Respir Med. 2014; 8:133–135. PMID: 24450398.15. Danila E, Norkūniene J, Jurgauskiene L, Malickaite R. Diagnostic role of BAL fluid CD4/CD8 ratio in different radiographic and clinical forms of pulmonary sarcoidosis. Clinical Respir J. 2009; 3:214–221. PMID: 20298407.
Article16. Hyldgaard C, Kaae S, Riddervold M, Hoffmann HJ, Hilberg O. Value of s-ACE, BAL lymphocytosis, and CD4+/CD8+ and CD103+CD4+/CD4+ T-cell ratios in diagnosis of sarcoidosis. Eur Respir J. 2012; 39:1037–1039. PMID: 22467726.
Article17. Winterbauer RH, Lammert J, Selland M, Wu R, Corley D, Springmeyer SC. Bronchoalveolar lavage cell populations in the diagnosis of sarcoidosis. Chest. 1993; 104:352–361. PMID: 8339618.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparative Analysis of Bronchoalveolar Lavages in Interstitial Lung Diseases
- Evaluation of CD3+CD4-CD8- (Double-negative) T Cells in Bronchoalveolar Lavage Fluid: an Effective Tool for Pulmonary Disease Diagnosis
- Analysis of Bronchoalveolar Lavage Fluid cells from the Patients of Diffuse Interstitial Lung Diseases
- Thoracoscopic Lung Biopsy for Diffuse Interstitial Lung Disease
- CD45 is Essential for Lymphocyte Gating in a T-lymphocyte Subset Assay of Bronchoalveolar Lavage Fluid by Flow Cytometry
