A Primary Sellar Neuroblastoma Mimicking a Pituitary Adenoma: A Case Report
- Affiliations
-
- 1Department of Radiology, Busan Paik Hospital, Inje University College of Medicine, Busan, Korea. youngjin726@hanmail.net
- 2Department of Pathology, Busan Paik Hospital, Inje University College of Medicine, Busan, Korea.
- KMID: 2360432
- DOI: http://doi.org/10.3348/jksr.2016.75.6.450
Abstract
- Intracranial neuroblastomas are uncommon malignant tumors that usually arise in the supratentorial parenchymal or paraventricular location. A primary neuroblastoma arising in the sella turcica is extremely rare. We report a case of a 76-year-old man who presented with progressive bitemporal hemianopsia. His pituitary hormone levels were within the normal range, except for slightly increased prolactin. Pituitary magnetic resonance imaging revealed a solitary sellar mass with supra- and parasellar extension that mimicked a non-functioning pituitary adenoma or meningioma. The tumor was excised by transsphenoidal resection. Histopathologic analysis revealed small cells surrounded by a dense fibrillary stroma as well as strong expression of neural markers. Hence, the patient was diagnosed with sellar neuroblastoma. Prolactin levels normalized in the immediate postoperative period, although visual disturbances persisted. Herein, we describe the clinical manifestations, MRI characteristics, and histopathologic findings of this case.
MeSH Terms
Figure
-
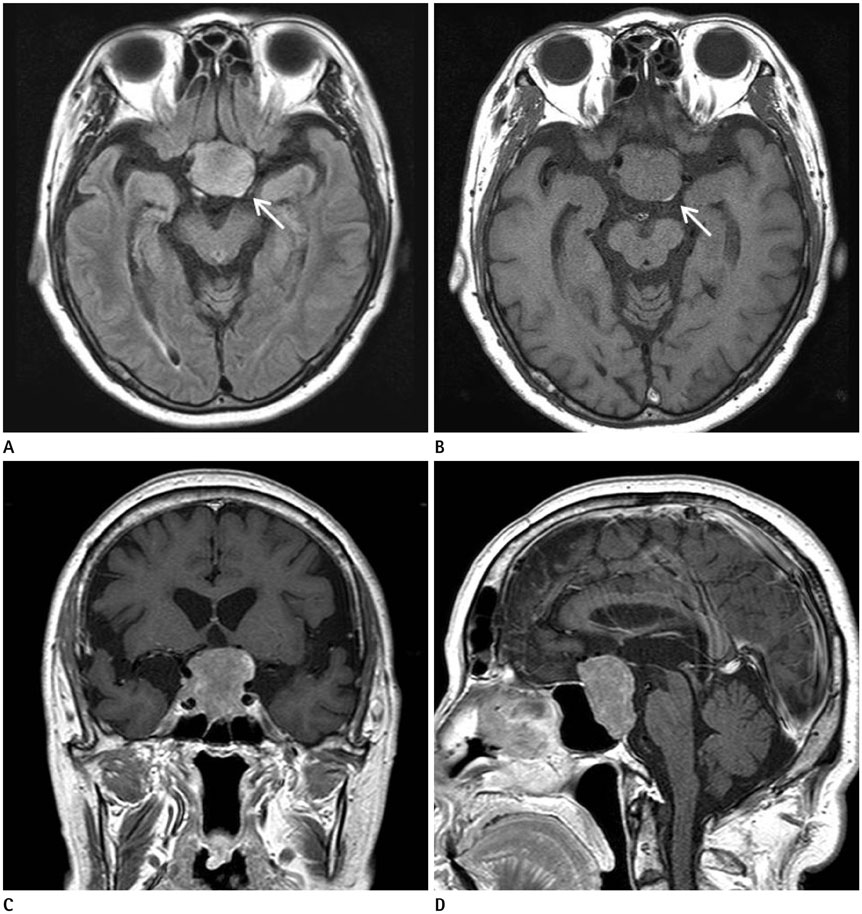
Fig. 1 A 76-year-old man with a primary sellar neuroblastoma. Axial fluid attenuation inversion recovery (FLAIR) magnetic resonance (MR) image (A) and T1-weighted MR image (B) show a homogeneous mass, with iso-signal intensity on T1-weighted image, and high signal intensity on FLAIR image with left posterolateral displacement of the neurohypophysis (arrows). Contrast-enhanced T1-weighted coronal (C) and sagittal (D) MR images show a well-enhancing large sellar mass with supra- and parasellar extension. Furthermore, there is no evidence of abnormalities in the paranasal sinuses or the floor of the sella turcica.
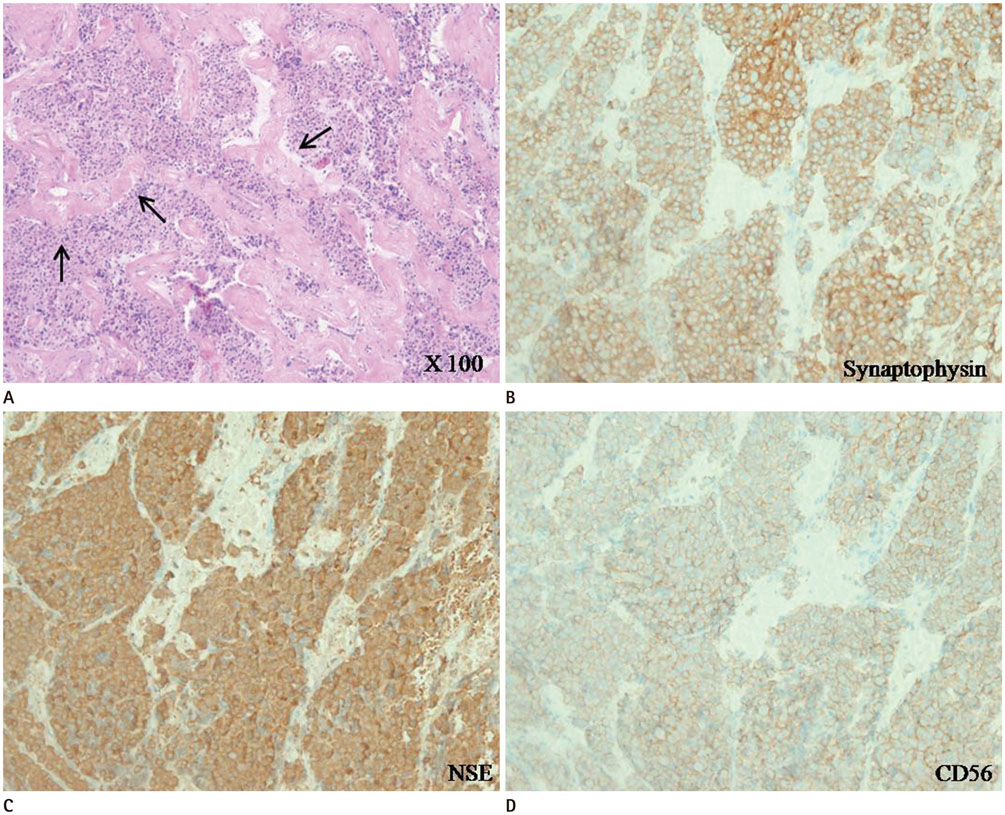
Fig. 2 Histopathologic examination of the excised sellar mass. Hematoxylin and eosin staining (A: magnification × 100) reveals tumor lobules separated by dense fibromuscular tissue (arrows). The neoplastic cells have small, round, inconspicuous nuclei, scant cytoplasm, and dispersed coarse to fine nuclear chromatin. Nuclear pleomorphism is substantial but mitotic activity and necrosis is absent. Neural markers (B: Synaptophysin, C: neuron-specific enolase, and D: neural cell-adhesion molecule/CD56, magnification × 200) show strong positive staining.
Reference
-
1. Schmalisch K, Psaras T, Beschorner R, Honegger J. Sellar neuroblastoma mimicking a pituitary tumour: case report and review of the literature. Clin Neurol Neurosurg. 2009; 111:774–778.2. Davis PC, Wichman RD, Takei Y, Hoffman JC Jr. Primary cerebral neuroblastoma: CT and MR findings in 12 cases. AJNR Am J Neuroradiol. 1990; 11:115–120.3. Dupuy M, Bonneville F, Grunenwald S, Breibach F, Delisle MB, Chaynes P, et al. Primary sellar neuroblastoma. A new case and review of literature. Ann Endocrinol (Paris). 2012; 73:216–221.4. Dulguerov P, Allal AS, Calcaterra TC. Esthesioneuroblastoma: a meta-analysis and review. Lancet Oncol. 2001; 2:683–690.5. Sarwar M. Primary sellar-parasellar esthesioneuroblastoma. AJR Am J Roentgenol. 1979; 133:140–141.6. Roy A, Timothy J, Anthony R, Chakrabarty A. Correspondence: aesthesioneuroblastoma arising in pituitary gland. Neuropathol Appl Neurobiol. 2000; 26:177–179.7. Frierson HF Jr, Ross GW, Mills SE, Frankfurter A. Olfactory neuroblastoma. Additional immunohistochemical characterization. Am J Clin Pathol. 1990; 94:547–553.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Pituitary Hyperplasia Secondary to Primary Hypothyroidism Mimicking Pituitary Tumor
- Sellar Tuberculoma Mimicking Pituitary Adenoma
- Sellar Chordoma Mimicking Pituitary Adenoma
- Pituitary Adenoma with Extensive Calcifications Mimicking Craniopharyngioma: A Case Report
- Pituitary Metastasis of Bronchial Carcinoid Tumor Mimicking Pituitary Adenoma: a Case Report
