A Pulmonary Sequestered Segment with an Aberrant Pulmonary Arterial Supply: A Case of Unique Anomaly
- Affiliations
-
- 1Department of Radiology, Eulji Hospital, Eulji University, Seoul 01830, Korea. jjblue@eulji.ac.kr
- KMID: 2360218
- DOI: http://doi.org/10.3348/kjr.2016.17.2.302
Abstract
- We presented a rare case of a 64-year-old man with a combined anomaly of the bronchus and pulmonary artery that was detected incidentally. Computed tomography showed a hyperlucent, aerated sequestered segment of the right lower lung with an independent ectopic bronchus, which had no connection to the other airway. The affected segment was supplied by its own aberrant pulmonary artery branch from the right pulmonary trunk. This anomaly cannot be classified with any of the previously reported anomalies.
MeSH Terms
Figure
-
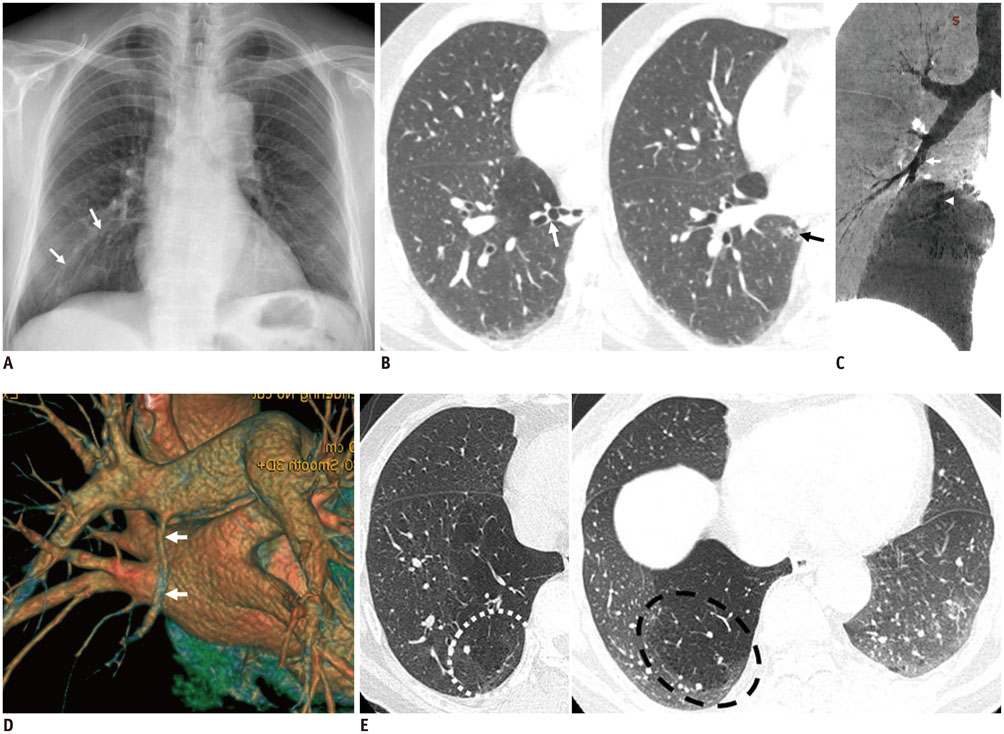
Fig. 1 Pulmonary sequestered segment with aberrant pulmonary arterial supply in 64-year-old man. A. 64-year-old man with hyperlucent right lower lobe (arrows). B. Lung window CT at full inspiration shows hyperlucent abnormal lung parenchyma located in lower medial zone of right lower lobe. White arrow (image on left) indicates tortous bronchiectatic bronchus and black arrow (image on right) indicates peripheral bronchiolectasia with bubbly appearance, connected to ectopic bronchus. C. Oblique coronal minimal intensity projection reconstruction shows proximal obliteration of right lower lobe segmental bronchus (arrow) and no visible communication between bronchial tree and ectopic bronchus (arrowhead) in hyperlucent lung. D. Three-dimensional volume rendering image shows anomalous segmental right pulmonary artery (arrows) arising from posteroinferior aspect of right pulomonary trunk. E. HRCT taken in inspiratory (image on left) and expiratory (image on right) phases. There are multiple small cyst-like or emphysematous lesions (in dotted line) in peripheral zone of affected hyperlucent segment. In expiratory phase HRCT, airtrapping in affected area is prominent, in comparison with normal contralateral lung. HRCT = high-resolution CT
Reference
-
1. Panicek DM, Heitzman ER, Randall PA, Groskin SA, Chew FS, Lane EJ Jr, et al. The continuum of pulmonary developmental anomalies. Radiographics. 1987; 7:747–772.2. Ferretti GR, Jouvan FB, Coulomb M. MDCT demonstration of intralobar pulmonary sequestration of the right upper lobe in an adult. AJR Am J Roentgenol. 2005; 185:1663–1664.3. Stern EJ, Webb WR, Warnock ML, Salmon CJ. Bronchopulmonary sequestration: dynamic, ultrafast, high-resolution CT evidence of air trapping. AJR Am J Roentgenol. 1991; 157:947–949.4. Ikezoe J, Murayama S, Godwin JD, Done SL, Verschakelen JA. Bronchopulmonary sequestration: CT assessment. Radiology. 1990; 176:375–379.5. Culiner MM, Wall CA. Collateral ventilation in "Intralobar pummonary sequestration." Report of a case. Dis Chest. 1965; 47:118–122.6. Cory RA, Valentine EJ. Varying patterns of the lobar branches of the pulmonary artery. A study of 524 lungs and lobes seen at operation of 426 patients. Thorax. 1959; 14:267–280.7. deMello DE, Sawyer D, Galvin N, Reid LM. Early fetal development of lung vasculature. Am J Respir Cell Mol Biol. 1997; 16:568–581.8. Hall SM, Hislop AA, Pierce CM, Haworth SG. Prenatal origins of human intrapulmonary arteries: formation and smooth muscle maturation. Am J Respir Cell Mol Biol. 2000; 23:194–203.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anomalous Systemic Arterial Supply to Normal Basal Segments of Left Lower Lobe: A Report of Two Cases
- Intralobar pulmonary sequestration with aberrant systemic artery - pulmonary vein fistula
- Anomalous systemic arterial supply to lung without sequestration in an infant who has congenital heart disease: a case report
- Aberrant Origin of the Upper Left Lobe Anterior and Superior Lingular Segmental Pulmonary Artery Arising from the Right Pulmonary Artery: A Case Report
- Superior Mediastinal Mass Revealed as Bronchopulmonary Sequestration Supplied by a Branch of the Left Pulmonary Artery
