Recurrent Carotid Cavernous Fistula Originating from a Giant Cerebral Aneurysm after Placement of a Covered Stent
- Affiliations
-
- 1Department of Neurosurgery, Busan Paik Hospital, Inje University, School of Medicine, Busan, Korea. kimst015@hanmail.net
- 2Department of Diagnostic Radiology, Busan Paik Hospital, Inje University, School of Medicine, Busan, Korea.
- 3Department of Neurology, Busan Paik Hospital, Inje University, School of Medicine, Busan, Korea.
- KMID: 2355660
- DOI: http://doi.org/10.7461/jcen.2016.18.3.306
Abstract
- We report the case of a recurrent carotid cavernous fistula (CCF) originating from a giant cerebral aneurysm (GCA) after placement of a covered stent. A 47-year-old woman presented with sudden onset of severe headache, and left-sided exophthalmos and ptosis. Cerebral angiography revealed a CCF caused by rupture of a GCA in the cavernous segment of the left internal carotid artery. Two covered stents were placed at the neck of the aneurysm. The neurological symptoms improved at first, but were aggravated in the 6 months following the treatment. Contrast agent endoleak was seen in the distal area of the stent. Even though additional treatments were attempted via an endovascular approach, the CCF could not be cured. However, after trapping the aneurysm using coils and performing superficial temporal artery-middle cerebral artery bypass, the neurological symptoms improved. In cases of recurrent CCF originating from a GCA after placement of a covered stent, it is possible to treat the CCF by endovascular trapping and surgical bypass.
MeSH Terms
Figure
-
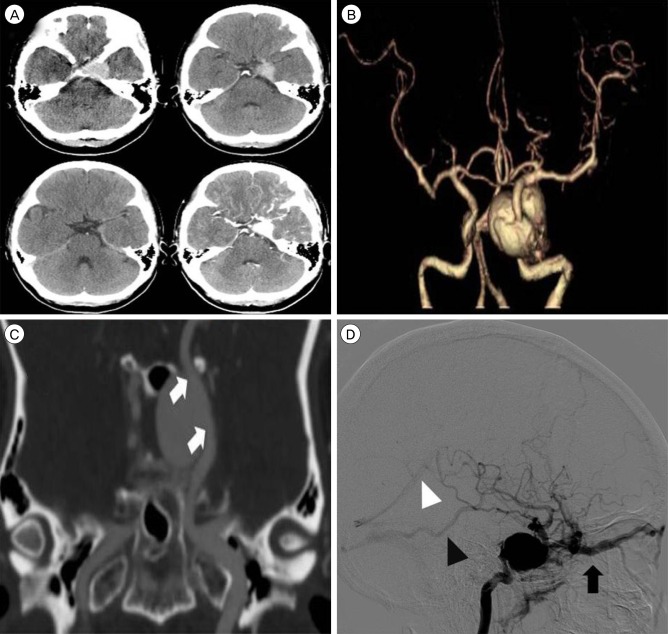
Fig. 1 Brain computed tomography (CT) angiography and transfemoral cerebral angiography. (A) Axial image of brain CT reveals a well-enhanced lesion in the left cavernous sinus. (B) Three-dimensional (3D) CT angiography reveals a giant cerebral aneurysm in a cavernous internal carotid artery (ICA). (C) The location and shape of the aneurysm can be seen in a coronal source image on CT angiography (white arrows indicate the proximal and distal neck of the aneurysm). (D) Lateral view of the left ICA by digital subtraction angiography reveals venous reflux of arterial blood flow. The block arrow indicates venous reflux through the superior ophthalmic vein. Black and white arrowheads indicate venous reflux through the vein of Labbé and the straight sinus, respectively.
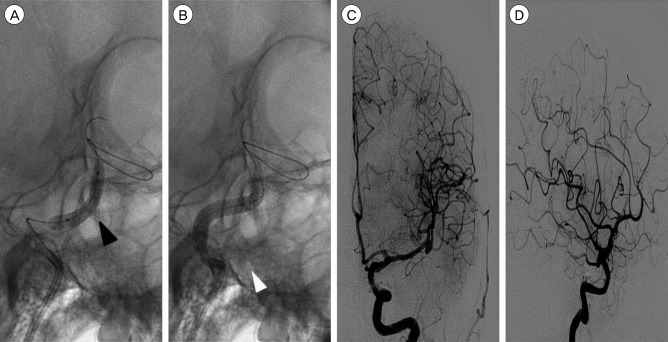
Fig. 2 (A) A 3.5 mm × 19 mm covered stent was placed in the cavernous internal carotid artery (ICA) between the anterior genu and the horizontal segment. Balloon angioplasty was performed, with inflation up to 20 atm (black arrowhead). (B) A 4 mm × 19 mm covered stent was placed in the cavernous ICA proximal to the previous deployed stent. Balloon angioplasty was performed, with inflation up to 24 atm (white arrowhead). (C, D) Follow-up left ICA angiography reveals disappearance of the aneurysm and the fistula. Anterograde blood flow to the left cerebral hemisphere can be clearly seen.
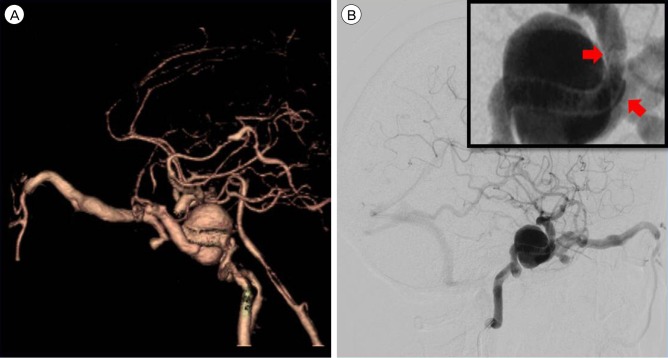
Fig. 3 (A) Computed tomography (CT) angiography after 6 months reveals recurrence of the giant aneurysm and carotid cavernous fistula. (B) In the lateral view on cerebral angiography, venous reflux can be seen to occur through the superior ophthalmic vein and cerebral cortical vein. A gap can be seen between the anterior genu of the ICA and the covered stent in a close-up view. ICA = internal carotid artery.
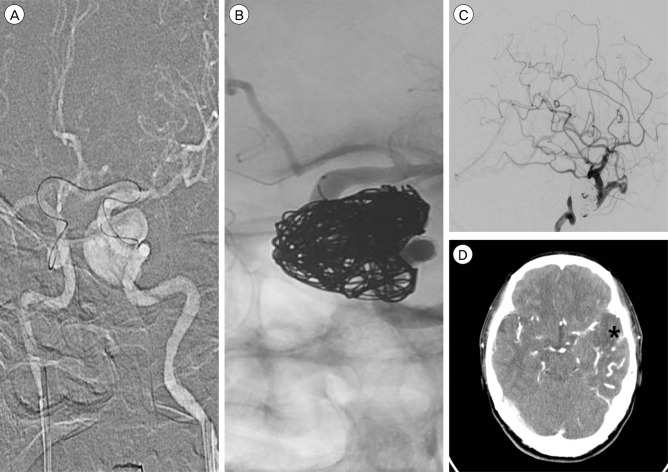
Fig. 4 Image taken during the second endovascular treatment. (A) The microcatheter can be seen entering the left distal internal carotid artery (ICA) via an A-Com channel, approaching from the right ICA, attempting to enter into the aneurysm through the gap between the stent and the ICA. (B) The aneurysm is packed using coils. However, the lower part of the aneurysm remained insufficiently packed. (C) In follow-up angiography, after coiling, reflux to the superior ophthalmic vein is found to be reduced. However, cortical venous reflux still exists. (D) On brain CT, low density and venous engorgement can be seen in the left temporal lobe. The asterisk indicates the infarct lesion. CT = computed tomography.
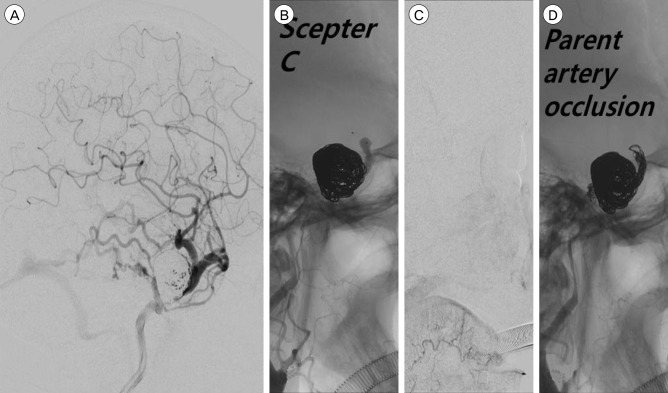
Fig. 5 Image obtained during the third endovascular treatment. (A) Cerebral angiography image obtained at 10 days after the previous treatment. Compared with the previous angiography, cortical venous reflux appeared to have increased. (B, C) After occluding the distal covered stent to the ophthalmic artery by means of a Scepter C balloon, angiography shows choroidal and disappearance of the CCF. (D) Angiography demonstrates complete occlusion of the ICA from the region proximal to the stent to the region distal to the ophthalmic artery. CCF = carotid cavernous fistula; ICA = internal carotid artery.
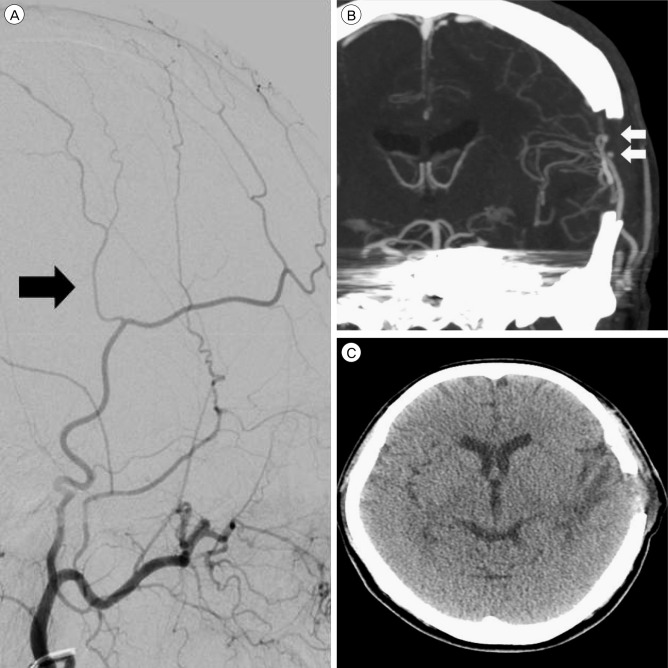
Fig. 6 Superficial temporal artery (STA) middle cerebral artery (MCA) bypass-related images. (A) Upon external carotid artery angiography, the caliber of the parietal branch seems smaller than that of the frontal branch (black arrow indicates parietal branch of the STA). (B) Coronal image taken during brain CTA reveals a patent double-barrel STA MCA bypass (white arrows indicate two anastomosis points). (C) A brain CT taken after 1 week reveals low density in the left temporal lobe that was thought to reflect the sequelae of a venous infarction. CTA = computered tomography angiography.
Reference
-
1. Archondakis E, Pero G, Valvassori L, Boccardi E, Scialfa G. Angiographic follow-up of traumatic carotid cavernous fistulas treated with endovascular stent graft placement. AJNR Am J Neuroradiol. 2007; 2. 28(2):342–347. PMID: 17297009.2. Bonello L, Tantry US, Marcucci R, Blindt R, Angiolillo DJ, Becker R, et al. Consensus and future directions on the definition of high on-treatment platelet reactivity to adenosine diphosphate. J Am Coll Cardiol. 2010; 9. 56(12):919–933. PMID: 20828644.
Article3. Delgado Almandoz JE, Crandall BM, Scholz JM, Fease JL, Anderson RE, Kadkhodayan Y, et al. Last-recorded P2Y12 reaction units value is strongly associated with thromboembolic and hemorrhagic complications occurring up to 6 months after treatment in patients with cerebral aneurysms treated with the pipeline embolization device. AJNR Am J Neuroradiol. 2014; 1. 35(1):128–135. PMID: 23828107.
Article4. Delgado Almandoz JE, Kadkhodayan Y, Crandall BM, Scholz JM, Fease JL, Tubman DE. Variability in initial response to standard clopidogrel therapy, delayed conversion to clopidogrel hyper-response, and associated thromboembolic and hemorrhagic complications in patients undergoing endovascular treatment of unruptured cerebral aneurysms. J Neurointerv Surg. 2014; 12. 6(10):767–773. PMID: 24353331.
Article5. dos Santos ML, Spotti AR, dos Santos RM, Borges MA, Ferrari AF, Colli BO, et al. Giant intracranial aneurysms: Morphology and clinical presentation. Neurosurg Rev. 2013; 1. 36(1):117–122. discussion 122. PMID: 22791075.
Article6. Eddleman CS, Surdell D, Miller J, Shaibani A, Bendok BR. Endovascular management of a ruptured cavernous carotid artery aneurysm associated with a carotid cavernous fistula with an intracranial self-expanding microstent and hydrogel-coated coil embolization: Case report and review of the literature. Surg Neurol. 2007; 11. 68(5):562–567. discussion 567. PMID: 17961748.
Article7. Geisler T, Zurn C, Simonenko R, Rapin M, Kraibooj H, Kilias A, et al. Early but not late stent thrombosis is influenced by residual platelet aggregation in patients undergoing coronary interventions. Eur Heart J. 2010; 1. 31(1):59–66. PMID: 19812059.
Article8. Gomez F, Escobar W, Gomez AM, Gomez JF, Anaya CA. Treatment of carotid cavernous fistulas using covered stents: Midterm results in seven patients. AJNR Am J Neuroradiol. 2007; 10. 28(9):1762–1768. PMID: 17885249.
Article9. Kobayashi N, Miyachi S, Negoro M, Suzuki O, Hattori K, Kojima T, et al. Endovascular treatment strategy for direct carotid-cavernous fistulas resulting from rupture of intracavernous carotid aneurysms. AJNR Am J Neuroradiol. 2003; 10. 24(9):1789–1796. PMID: 14561604.10. Kupersmith MJ, Hurst R, Berenstein A, Choi IS, Jafar J, Ransohoff J. The benign course of cavernous carotid artery aneurysms. J Neurosurg. 1992; 11. 77(5):690–693. PMID: 1403108.
Article11. Lewis AI, Tomsick TA, Tew JM Jr. Management of 100 consecutive direct carotid-cavernous fistulas: Results of treatment with detachable balloons. Neurosurgery. 1995; 2. 36(2):239–244. discussion 244-5. PMID: 7731502.12. Li K, Cho YD, Kim KM, Kang HS, Kim JE, Han MH. Covered stents for the endovascular treatment of a direct carotid cavernous fistula : Single center experiences with 10 cases. J Korean Neurosurg Soc. 2015; 1. 57(1):12–18. PMID: 25674338.
Article13. Polin RS, Shaffrey ME, Jensen ME, Braden L, Ferguson RD, Dion JE, et al. Medical management in the endovascular treatment of carotid-cavernous aneurysms. J Neurosurg. 1996; 5. 84:755–761. PMID: 8622148.
Article14. Sibbing D, Morath T, Braun S, Stegherr J, Mehilli J, Vogt W, et al. Clopidogrel response status assessed with multiplate point-of-care analysis and the incidence and timing of stent thrombosis over six months following coronary stenting. Thromb Haemost. 2010; 1. 103(1):151–159. PMID: 20062919.
Article15. Sugawara Y, Kikuchi T, Ueda T, Nishizaki M, Nakata S, Mochizuki T, et al. Usefulness of brain SPECT to evaluate brain tolerance and hemodynamic changes during temporary balloon occlusion test and after permanent carotid occlusion. J Nucl Med. 2002; 12. 43(12):1616–1623. PMID: 12468510.16. Tiewei Q, Ali A, Shaolei G, Feng L, Zhongsong S, Xuesong L, et al. Carotid cavernous fistulas treated by endovascular covered stent grafts with follow-up results. Br J Neurosurg. 2010; 8. 24(4):435–440. PMID: 20515263.
Article17. van Rooij WJ, Sluzewski M, Beute GN. Ruptured cavernous sinus aneurysms causing carotid cavernous fistula: Incidence, clinical presentation, treatment, and outcome. AJNR Am J Neuroradiol. 2006; 1. 27(1):185–189. PMID: 16418380.18. van Rooij WJ, Sluzewski M, Metz NH, Nijssen PC, Wijnalda D, Rinkel GJ, et al. Carotid balloon occlusion for large and giant aneurysms: Evaluation of a new test occlusion protocol. Neurosurgery. 2000; 7. 47(1):116–121. discussion 122. PMID: 10917354.
Article19. van Rooij WJ, Sluzewski M, Slob MJ, Rinkel GJ. Predictive value of angiographic testing for tolerance to therapeutic occlusion of the carotid artery. AJNR Am J Neuroradiol. 2005; 1. 26(1):175–178. PMID: 15661722.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Carotid-Cavernous Fistula Due to Giant Aneurysm in a Postpartum Woman
- Treatment of carotid-carvenous fistula and internal carotid aneurysm with Latex detachable balloons
- Regional Cerebral Blood Flow Changes in Traumatic Carotid Cavernous Fistula During Trapping Procedure: Case Study, Preliminary Report
- Treatment of Carotid-Cavernous Fistula and Internal Carotid Aneurysm with Debrun's Latex Detachable Balloon Catheter Technique
- Treatment of High-Flow Carotid Cavernous Fistula Using a Graft Stent: Case Report
