Surgical Outcomes after Olecranon Plating with Retrograde Coronoid Process Screw Fixation through the Plate Hole in the Bifocal Fracture of the Proximal Ulna
- Affiliations
-
- 1Department of Orthopedic Surgery, CHA Bundang Medical Center, CHA University, Seongnam, Korea. hsoohong@daum.net
- 2Department of Orthopedic Surgery, CHA Gumi Medical Center, CHA University, Gumi, Korea.
- KMID: 2355505
- DOI: http://doi.org/10.4055/jkoa.2016.51.5.403
Abstract
- PURPOSE
Bifocal fracture of the proximal ulna is a fracture of the olecranon accompanied by fracture of the coronoid process. The purpose of the current study was to analyze the clinical results of the author's technique in bifocal fracture of the proximal ulna.
MATERIALS AND METHODS
Fifteen patients (10 men, 5 women) treated at CHA Bundang Medical Center from April 2006 to October 2014 were analyzed retrospectively. All patients underwent internal fixation using a locking compression plate (LCP) with retrograde screw fixation of the coronoid process through a screw hole of the plate. Mean age of the patients was 42.6 years and the mean follow-up period was 18.6 months. Comminuted coronoid fractures with hard to screw fixation, complex injuries combined with open damage, and complete ligament rupture were excluded. Fracture union and articular congruity were examined on the follow-up radiographs. Range of motion, disability of the arm, shoulder and hand (DASH) score, and Mayo elbow performance score were evaluated for functional analysis.
RESULTS
Fracture union was achieved and articular step off was less than 2 mm in all patients on the follow-up radiographs. The mean value of modified Mayo elbow score was 92.14 (80-100) and DASH score was 7.11 at last follow-up. The mean range of motion of elbow was 128o. There was one case of small heterotopic ossification as a radiographic complication which had no functional deficit.
CONCLUSION
Internal fixation of bifocal multifragmentary articular fractures of the proximal ulna with anatomically contoured LCP olecranon plate and retrograde long screws could be a recommendable surgical procedure. This study showed that the precontoured plate with retrograde coronoid process screw fixation can produce good clinical and radiographic outcomes in bifocal fractures of the proximal ulna. We recommend this procedure in this type of fracture.
MeSH Terms
Figure
-
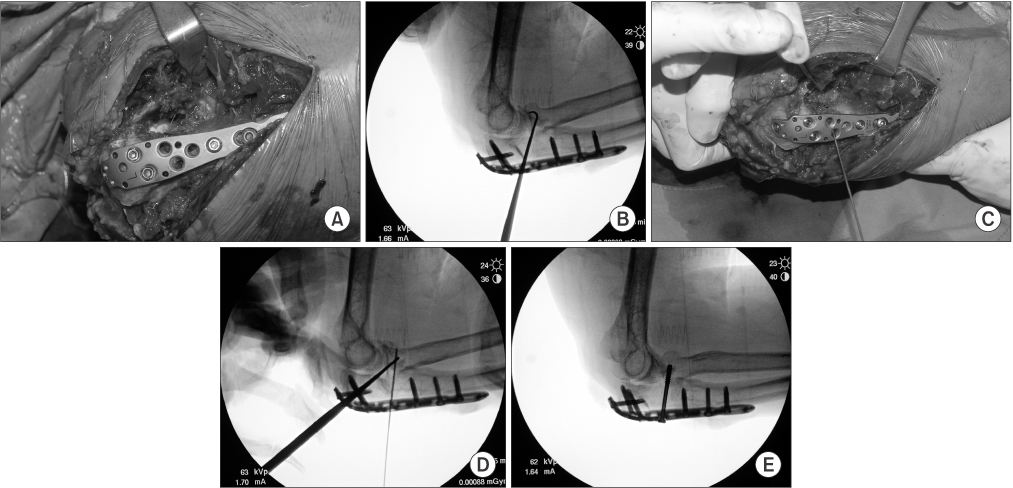
Figure 1 Intraoperative view. (A) The olecranon was initially fixed with a 3.5 mm anatomically contoured locking compression plate. (B-D) After fixation of the olecranon, the gap of the coronoid process fragment was checked with using an image intensifier. In cases of more than 2 mm of gap, the coronoid process was indirectly reduced with using a bone hook and provisional fixation with K-wire was performed done. (E) Retrograde fixation of the coronoid process was performed done using a long screw through a screw hole of the plate.
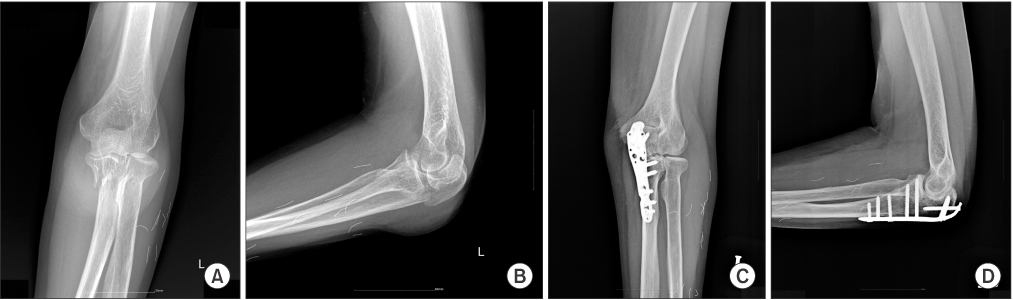
Figure 2 Pre- and postoperative imaging study. (A, B) Comminuted olecranon fracture and associated coronoid process fracture were seen observed on anteroposterior and lateral view. (C, D) The anteroposterior and lateral view at 12 months after the operation show good healing of the fracture.

Figure 3 Postoperative photographs. The photographs show a good functional result of an injured elbow with nearly normal range of motion equivalent to non-injured elbow.

Figure 4 Pre- and postoperative radiographs. (A, B) Comminuted olecranon fracture and associated coronoid process fracture were seen observed on anteroposterior and lateral view. (C, D) The anteroposterior and lateral view at 18 months after the operation show good healing of the fracture.

Figure 5 Postoperative photographs. The photographs show a good functional result of an injured elbow with nearly normal range of motion equivalent to the non-injured elbow.
Reference
-
1. Müller ME, Allgöwer M, Schneider R, Willenegger H. Manual of internal fixation: techniques recommended by the AOASIF group. 3rd ed. Berlin: New York: Springer-Verlag;1991.2. Fyfe IS, Mossad MM, Holdsworth BJ. Methods of fixation of olecranon fractures. An experimental mechanical study. J Bone Joint Surg Br. 1985; 67:367–372.
Article3. Simpson NS, Goodman LA, Jupiter JB. Contoured LCDC plating of the proximal ulna. Injury. 1996; 27:411–417.
Article4. Veillette CJ, Steinmann SP. Olecranon fractures. Orthop Clin North Am. 2008; 39:229–236. vii
Article5. Isik Ç, Tahta M, Aksekili MAE, et al. Retrograde screw fixation results of coronoid fractures in terrible triad. Br J Med Med Res. 2015; 8:802–805.
Article6. Rhee YG, Cha JR. The role of the coronoid process fracture in the elbow dislocation. J Korean Soc Fract. 2001; 14:491–498.
Article7. Boyer MI, Galatz LM, Borrelli J Jr, Axelrod TS, Ricci WM. Intra-articular fractures of the upper extremity: new concepts in surgical treatment. Instr Course Lect. 2003; 52:591–605.8. Wells J, Ablove RH. Coronoid fractures of the elbow. Clin Med Res. 2008; 6:40–44.
Article9. Moon JG, Zobitz ME, An KN, O'Driscoll SW. Optimal screw orientation for fixation of coronoid fractures. J Orthop Trauma. 2009; 23:277–280.
Article10. Buijze G, Kloen P. Clinical evaluation of locking compression plate fixation for comminuted olecranon fractures. J Bone Joint Surg Am. 2009; 91:2416–2420.
Article11. Melamed E, Danna N, Debkowska M, Karia R, Liporace F, Capo JT. Complex proximal ulna fractures: outcomes of surgical treatment. Eur J Orthop Surg Traumatol. 2015; 25:851–858.
Article12. Niglis L, Bonnomet F, Schenck B, et al. Critical analysis of olecranon fracture management by pre-contoured locking plates. Orthop Traumatol Surg Res. 2015; 101:201–207.
Article13. Mouhsine E, Akiki A, Castagna A, et al. Transolecranon anterior fracture dislocation. J Shoulder Elbow Surg. 2007; 16:352–357.
Article14. Morrey BF, An KN. Stability of the elbow: osseous constraints. J Shoulder Elbow Surg. 2005; 14:174S–178S.
Article15. Hak DJ, Golladay GJ. Olecranon fractures: treatment options. J Am Acad Orthop Surg. 2000; 8:266–275.
Article16. Horner SR, Sadasivan KK, Lipka JM, Saha S. Analysis of mechanical factors affecting fixation of olecranon fractures. Orthopedics. 1989; 12:1469–1472.
Article17. Morrey BF. The elbow and its disorders. 2nd ed. Philadelphia: WB Saunders;1993. p. 19.18. Karlsson MK, Hasserius R, Besjakov J, Karlsson C, Josefsson PO. Comparison of tension-band and figure-of-eight wiring techniques for treatment of olecranon fractures. J Shoulder Elbow Surg. 2002; 11:377–382.
Article19. Tashjian RZ, Katarincic JA. Complex elbow instability. J Am Acad Orthop Surg. 2006; 14:278–286.
Article20. Doornberg JN, Ring DC. Fracture of the anteromedial facet of the coronoid process. J Bone Joint Surg Am. 2006; 88:2216–2224.
Article21. Shin DJ, Byun YS, Cho YH, Park HW, Youn HM, Han JH. Plate fixation for fractures of the coronoid process of the ulna. J Korean Shoulder Elbow Soc. 2008; 11:177–184.
Article22. Cho JH, Kim JY, Lee DH, Han KJ. Surgical treatment of transolecranon fracture-subluxation of the elbow. J Korean Soc Surg Hand. 2008; 13:200–204.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Plate Fixation for Fractures of the Coronoid Process of the Ulna
- The Challenge of Trans-Ulnar Basal Coronoid Fracture-Dislocations: A Surgical Strategy Based on the Pattern of Coronoid Fracture
- Tension Band Fixation in the Treatment of the Olecranon Fracture
- The Surgical Outcomes of Olecranon Fracture Dislocation of the Elbow
- Reconstruction of the coronoid process using a graft from the olecranon of the same side for chronic posterior dislocation of the elbow
